| How to cite this article
Makama JG, Garba ES, Amedh EA. Under Representation of Women in Surgery in Nigeria: By Choice or by Design? Oman Med J 2012 Jan; 27(1):66-69.
How to cite this URL
Makama JG, Garba ES, Amedh EA. Under Representation of Women in Surgery in Nigeria: By Choice or by Design? Oman Med J 2012 Jan; 27(1):66-69. Available from http://www.omjournal.org/fultext_PDF.aspx?DetailsID=200&type=fultext
Abstract
Background: Female Doctors’ lack of interest in surgical careers has raised much concern in recent times. An understanding of the factors responsible for this lack of interest and evolving attitude is needed. The aim of this report was to determine the local factors that may be responsible and the most likely surgical specialty female doctors would prefer.
Methods: This is a cross sectional study involving all female (consultant and resident) doctors in one teaching hospital. Information was obtained using a structured questionnaire which determined what formed the respondent’s choice of present specialty. It also included the likely local factors that might have some bearings on the interest of female doctors in surgery. Data obtained were analyzed using SPSS version 11.5.
Results: There were a total of 105 respondents. The age range was26 - 63 years (mean: 26.88+2.19). The factors that were considered as deterrents to female doctor choice of surgical career were: a)the impact on their time for family and other social engagements 29 (27.6%); b) heavy work load 22 (21%); c) involvement of a lot of physical effort 18 (17.1%); d) lack of women in surgery 9 (8.6%); and e) lack of role models 4 (3.8%). Twenty three (21.9%) considered all the above factors. The subspecialty preferred by most female was plastic and reconstructive surgery, followed by Pediatric surgery.
Conclusion: The rigorous requirements of the training and practice of surgery deterred female doctors’ interest in choosingand sustaining a surgical career. To maintain surgery as a premier career choice, female doctors should find surgery to be professionally and personally rewarding.
Keywords: Female doctors; Surgical career; Challenges; Nigeria.
Introduction
In recent times, there has been a relative increase in the number of female medical students in most medical schools in USA.1,2 However, this has not been reflected in postgraduate residency training programs in surgery. Gender discrimination in surgical programs has been noted to be wide spread and flagrant.2 In Nigeria, there may not be any difference from what is reportedin USA. An understanding of the factors responsible for this is needed. The aim of this report is to determine whether under representation of women in surgery in Nigeria is by choice or by design. The most likely surgical specialty females can cope with and local factors that preclude female doctors’ interest in surgery will also be considered.
Methods
This was a cross sectional study (June - August, 2009), involving female doctors (both consultants and residents) in Ahmadu Bello University Teaching Hospital, Zaria, a tertiary teaching hospital located in the north central part of Nigeria. This study was conducted by the use of a structured questionnaire to obtain the necessary information. The questionnaire, which was anonymously administered, determined the respondent’sspecialty and what formed the choice of this present specialty. It also determined the likely local factors that may be perceived as deterrents to female doctors specializing in surgery; whether more females can be encouraged to take up surgical careers andthe subspecialty considered most suitable to cope with. At the time of the study there were only two female Residents in the Surgery Department. The questionnaires were administered by one of the authors (JGM).
A total of 115 questionnaires were given out (Consultants 37, Residents 78) and 105 were adequately completed and returned (Consultants 31, Residents 74). All data were imported into an SPSS Windows Version 11 spread sheet program for the purpose of generating frequency tables for variables. Statistical analysis was performed on all questions from the survey considered relevant tothe study. The chi-square test was used to test for proportions. The level of significance was set at 0.05 for all statistical tests.
Results
The response rate was 82% (105 of 115). The 105 respondents were aged 26 to 63 years (mean: 40.02+6.51). The distribution of respondents by specialty and status (Table 1, Fig. 1) revealed that the majority of the female doctors were in Obstetrics and Gynecology, 40 (39%); followed by Pediatric Medicine, 28(26.6%). Thirty one (29.5%) Consultants and 74 (70.5%) Residents participated in the study. The factors that formed the choice oftheir present specialty (Fig. 2) included the following: a) Personal interest (n=36; 34.3%); b) Attracted by role models (n=24; 22.8%);c) Loves to interact with the category of patients in the specialty (n=14; 13.3%); d) Influence of friends/peer group (n=13; 12.4%);e) Job pressure (n=11; 10.5%); and f) Chose this specialty for otherreasons (n=7; 6.7%).
While the factors that were considered as deterrents (Fig. 3) to female doctors from choosing a surgical career were: a) Limited or no time for family and other social engagements (n=29; 27.6%); b) Heavy work load (n=22; 21%); c) Involvement of a lot of physical effort (n=18; 17.1%); d) Lack of women in surgery (n=9; 8.6%);and e) Lack of role models (n=4; 3.8%). Twenty three participants(21.9%) considered all the above factors. All the participants agreed that more female doctors should be encouraged to take up surgical careers. The subspecialty considered most appropriate for female doctors was plastic and reconstructive surgery, followed by pediatric surgery. (Fig.4)
Table 1: Distribution of respondents by Specialty and status.


Figure 1: Distribution of female doctors by specialty and status.
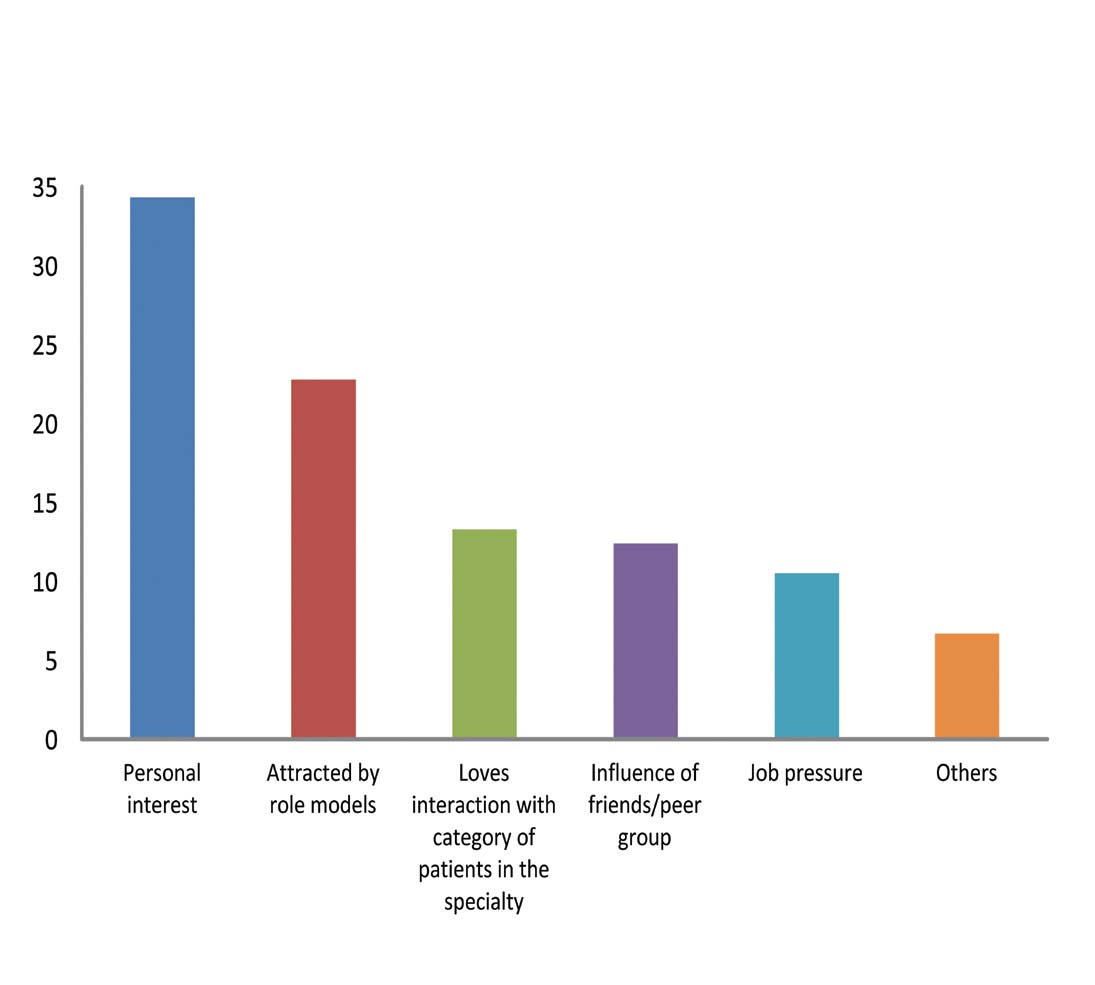
Figure 2: Factors that informed the choice of the present specialtydistribution.

Figure 3: Deterrents to choice of surgical career.

Figure 4: Subspecialty considered most appropriate for femalesurgeons.
Discussion
In the present report, only few of the female respondents werein Surgery Department either as surgeons or residents. The distribution of female doctors that have indicated interest in specialization in our center was mostly in Obstetrics and Gynaecology, and Pediatric medicine and most of the factors that influenced the choice included personal interest, the impact of role models, influence by friends/peer group and job pressure. Also in the present study, heavy workload and lack of time for family and social engagements were considered major deterrents to their interest in taking up a surgical career. Consequently, female doctors who would rather reserve their time for family and friends in their working lives, would be compelled to take up other medical specialties because of their manageable schedule; hence, no middle-of-the-night emergencies.3
Women are deterred from a career in surgery for substantially many reasons in our setting. This is evident by the fact that significant number 23 (22.%) of respondents considered all factors to be relevant in preventing female doctors from choosing surgery as a career. The surgical specialty considered most suitable for female doctors in our setting in this study was plastic and reconstructive surgery closely followed by pediatrics surgery.
The absence of other female doctors in surgery has made being a woman in such a field so difficult.3,4 This is a significant factor (being considered sex-specific), that does not only deter women,but has created a vicious cycle which requires urgent attention.3 The significance of this study is that it has unravelled important deterrents that prevent female doctors from choosing surgery asa career. Therefore, deliberate efforts to apprehend have to be inplace and should be encouraged so as to arrest the vicious cycle inour environment. Some reports have examined the factors that influence career choice among medical students and pre-registration house officers.2,3
Some of the factors that positively influenced careerchoice in surgery included the desire for a prestigious career, interest in performing procedures, desiring leadership roles ,and willingness to sacrifice lifestyle to obtain goals.2-5 However, lifestyle priorities of the current generation of doctors have been shown to have shifted the desire to choose surgery as a career.6,7 While other medical specialties have high female presence, women are still under represented in surgery.8,9
A relative increased enrollment of female medical students and thus female graduates have been noted in most medical schools in USA,10,11 but when time comes to applying for residency training, quite a number of them will shift their interest to Obstetrics and Gynecology, Pediatrics, Community or Family practice, Internal medicine, Psychiatry and Ophthalmology than Surgery.2,10,11 The flexibility in schedules and approach to training options have been considered to be major factors of interest in the other medical specialties.12,13 In the world of medicine, surgeons are considered highly trained and hard working elites.14 Many men outside of medicine as well as male physicians would rather have a more traditional wife who would have time to run a house and raise their family, given the enormous time demands on surgeons.15 This general need will continue to influence not only female doctors but also their spouses even when they are married.
Having role models has clearly been shown to be an important factor in choosing a surgical career.16-18 However, in our study, only a few women (3.8%) considered lack of role models as a deterrentto female interest in surgical careers. Whether female role models were necessary to influence their choice or not was not evaluated.
Strategies for correcting this imbalance may include affirmative recruitment of women into surgery, creation of female friendly support systems such as child care and adjustment of schedules to allow time for family and social engagements.19,20
A limitation of this study is the fact that the questionnaire was not administered to the respondents (female doctors) before and after commencement of residency programs. Also, the opinions of the male counter parts, as potential or real husbands to these female doctors could not be evaluated. This should be the focus of a follow up study.
Conclusion
The rigorous requirements of the training and practice of surgery deters female doctors’ interest in surgery. To maintain surgery as an attractive career choice, female doctors should find surgery tobe professionally and personally rewarding.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Evans S, Sarani B. The modern medical school graduate and general surgicaltraining: are they compatible? Arch Surg 2002 Mar;137(3):274-277.
2. Sanfey HA, Saalwachter-Schulman AR, Nyhof-Young JM, Eidelson B,Mann BD. Influences on medical student career choice: gender or generation?Arch Surg 2006 Nov;141(11):1086-1094, discussion 1094.
3. Debra A, Gargiulo MD, Neil H, Hyman MD, James C, Hebert MD.Women in surgery: Do we really understand the deterrents. Arch Surg2006;141:1086-1094.
4. Wendel TM, Godellas CV, Prinz RA. Are there gender differences inchoosing a surgical career? Surgery 2003 Oct;134(4):591-596, discussion596-598.
5. Baxter N, Cohen R, McLeod R. The impact of gender on the choice of surgeryas a career. Am J Surg 1996 Oct;172(4):373-376.
6. Dorsey ER, Jarjoura D, Rutecki GW. Influence of controllable lifestyleon recent trends in specialty choice by US medical students. JAMA 2003Sep;290(9):1173-1178.
7. Walters BC. Why don’t more women choose surgery as a career? Acad Med1993 May;68(5):350-351.
8. Neumayer L, Kaiser S, Anderson K, Barney L, Curet M, Jacobs D, et al.Perceptions of women medical students and their influence on career choice.Am J Surg 2002 Feb;183(2):146-150.
9. Blakemore LC, Hall JM, Biermann JS. Women in surgical residency trainingprograms. J Bone Joint Surg Am 2003 Dec;85-A(12):2477-2480.
10. Sonnad SS, Colletti LM. Issues in the recruitment and success of women inacademic surgery. Surgery 2002 Aug;132(2):415-419.
11. Colletti LM, Mulholland MW, Sonnad SS. Perceived obstacles to career success for women in academic surgery. Arch Surg 2000 Aug;135(8):972-977.
12. Weber T, Reidel M, Graf S, Hinz U, Keller M, Büchler MW. Careers ofwomen in academic surgery. Chirurg 2005 Jul;76(7):703-711, discussion 711.
13. Park J, Minor S, Taylor RA, Vikis E, Poenaru D. Why are women deterredfrom general surgery training? Am J Surg 2005 Jul;190(1):141-146.
14. Richard HC, Redtem N. Why women reject surgical careers? Annals of theRoyal College of England 2000;82:290-293
.15. Mackinnon SE, Mizgala CL, McNeill IY, Walters BC, Ferris LE. Womensurgeons: career and lifestyle comparisons among surgical subspecialties.Plast Reconstr Surg 1995 Feb;95(2):321-329.
16. Fysh TH, Thomas G, Ellis H. Who wants to be a surgeon? A study of 300first year medical students. BMC Med Educ 2007;7:2.
17. Nonnemaker L. Women physicians in academic medicine: new insights fromcohort studies. N Engl J Med 2000 Feb;342(6):399-405.
18. Hoover EL. Mentoring women in academic surgery: overcoming institutionalbarriers to success. J Natl Med Assoc 2006 Sep;98(9):1542-1545.
19. Carty SE, Colson YL, Garvey LS, Schuchert VD, Schwentker A, Tzeng E,et al. Maternity policy and practice during surgery residency: how we do it.Surgery 2002 Oct;132(4):682-687, discussion 687-688.
20. Kass RB, Souba WW, Thorndyke LE. Challenges confronting femalesurgical leaders: overcoming the barriers. J Surg Res 2006 May;132(2):179-187.
|