|
Introduction
The supraorbital nerve is one of the main cutaneous nerves supplying the forehead and scalp region. It exits through its foramen to innervate the skin and may be injured during various surgical and anesthetic procedures.1 The supraorbital nerve blocks are commonly performed in the region of supraorbital foramen during procedures such as closure of facial wounds, biopsies, and scar revisions, as absolute but temporary treatment for supraorbital neuralgia and other cosmetic cutaneous procedures. Effective and precise analgesia can be achieved only if one is aware of the most frequent location of exit of the nerve in this region.1,2 Knowledge of the location of this nerve is also essential during various endoscopic procedures, which are increasingly being used for cosmetic facial surgery.3,4 Excessive dissection and retraction close to such neurovascular bundles can cause scarring, which may lead to entrapment neuropathies and painful neuralgias.5,6 Clinicians must be aware of the exact position of SOF/SON while diagnosing conditions like supraorbital neuralgia, as it is normally characterized by forehead pain and tenderness over the SON/SOF.7
In this study, measurements were made on cadaveric dry skulls from South India to determine the location and dimensions of the supraorbital notch (SON) or the supraorbital foramen (SOF). Data obtained were compared with those from other races and regions. The data may be useful to anesthetists and surgeons for providing appropriate nerve blocks and planning the surgical flaps.
Methods
Eighty-three dry adult human skulls of unknown gender were used for the study. The skulls were collected from the Department of Anatomy, Melaka Manipal Medical College, Manipal, and from the Departments of Anatomy and Forensic Medicine, Kasturba Medical College, Manipal. The study was conducted between June 2009 and March 2011, and approval was obtained from the Institutional ethical committee before study commencement.
The skulls were measured bilaterally using “travelling Vernier’s microscope” precision- 10 µ, Sisco, New Delhi, India. In this study, the parameters studied were distance between the SOF or SON and the nasal midline, distance between the SOF or SON and the frontozygomatic suture, (Fig. 1); height of the supraorbital foramen that is vertical distance between the lowest point along the lower margin of the SOF and supra orbital margin; transverse diameter of supraorbital notch that is transverse distance between the lower ends of medial and lateral margins of the SON; the presence of accessory foramina, their number, location and distance from the main SON/SOF.
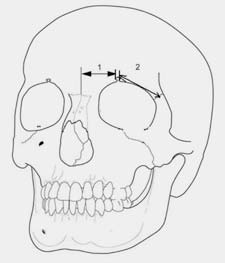
Figure 1: The measurements of the supraorbital notch/ foramen, in relation to important anatomical/surgical landmarks. “1” indicates the distance from supraorbital notch/foramen to nasal midline and “2” indicates the distance from the supraorbital notch/foramen to frontozygomatic suture.
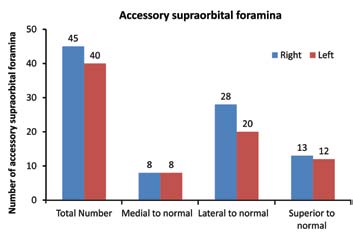
Figure 2: The number of accessory supraorbital foramina on right and left sides.
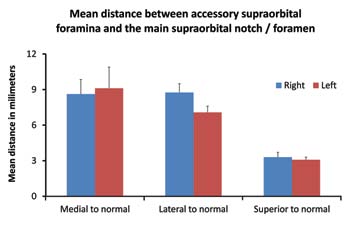
Figure 3: The mean distance between accessory supraorbital foramina and the main supraorbital notch/foramen on right and left sides. Mean distance of medial ASF from the main SOF/SON was 8.62±1.23 mm on the right side and 9.11±1.78 mm on the left side. Mean distance of lateral ASF from the main SOF/SON was 8.75±0.74 mm on the right side and 7.07±0.53 mm on the left side. Mean distance of superior ASF from the main SOF/SON was 3.3±0.41 mm on the right side and 3.08±0.22 mm on the left side.
Skulls which were damaged, fractured, deformed or with apparent abnormalities were excluded from the study. The data obtained were analyzed using the statistical software Graph Pad Prism version 3.00, GraphPad Software, Inc. San Diego CA and paired t-test was applied to analyze the difference between the data from right and left sides. Graphical representations of the data were obtained from Microsoft Excel 2007.
Results
The study of 83 adult skulls revealed that the SON (69.87%) was found more frequently than the SOF (28.91%). Of all the cases, 56.62% had bilateral SON, while 14.45% had bilateral SOF. Notches were mostly observed on the right side and foramina were mostly seen on the left side. The mean distance between the right and left SON/SOF and the nasal midline; mean distance between right and left SON/SOF and frontozygomatic sutures; mean height of right and left SOF; and the mean transverse diameter of right and left SON are shown in Table 1. When these parameters were compared between the right and left sides, there was no statistically significant difference.
Table 1: Location and dimensions of the supraorbital foramen and supraorbital notch.
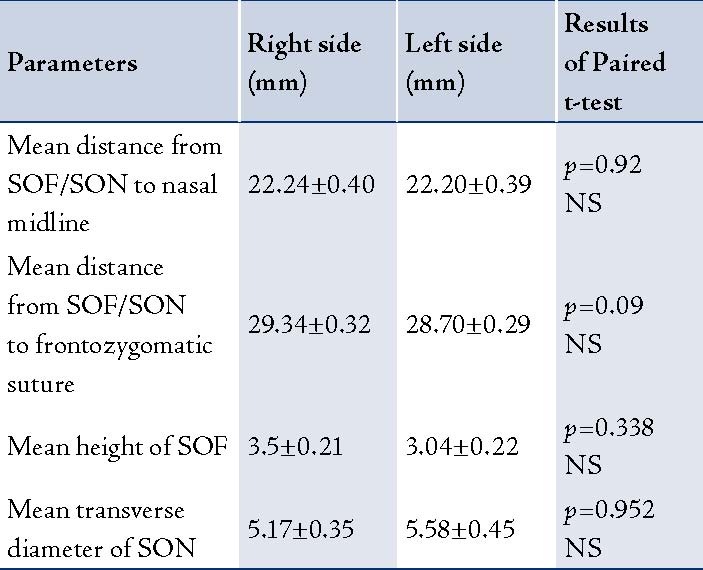
It can be noted that the results of comparison between the two sides is not significant in all the parameters. (SOF- supraorbital foramen; SON- supraorbital notch; NS- not significant)
Fifty five (66.25%) skulls showed accessory supraorbital foramina (ASF). Of these, 30 (54.54%) skulls had ASF on both sides, while 25 (45.45%) only had ASF on one side and in 28 (33.73%) skulls, ASF were completely absent. On right side, 8 (17.77%) accessory supraorbital foramina were seen medial, 28 (62.2%) were observed lateral and 13 (28.88%) were found superior to the main SON/SOF. On left side, 8 (20%) accessory supraorbital foramina were observed medial, 20 (40%) were located lateral and 12 (30%) were found superior to the main SON/SOF, (Fig. 2). The mean distance of medial ASF from the main SOF/SON was 8.62±1.23 mm on the right side and 9.11±1.78 mm on the left side. The mean distance of lateral ASF from the main SOF/SON was 8.75±0.74 mm on the right side and 7.07±0.53 mm on the left side. While the mean distance of superior ASF from the main SOF/SON was 3.3±0.41 mm on the right side and 3.08±0.22 mm on the left side. (Fig. 3)
Discussion
Normally, the supraorbital notch (SON) or supraorbital foramen (SOF) is situated along the supraorbital margin, which is entirely formed by the frontal bone. The supraorbital margin is interrupted at the junction of its sharp lateral two-thirds and rounded medial one-third by the supraorbital notch or foramen. Supraorbital notch or foramen transmits supraorbital nerve and vessels. Supraorbital nerve is the larger terminal branch of the frontal nerve, which is a branch of ophthalmic division of trigeminal nerve and it traverses through the SON/SOF and divides into medial and lateral branches to supply the palpebral filaments to the upper eyelid, conjunctiva and skin of the scalp as far back as the lambdoid suture. Supraorbital artery is a branch from the ophthalmic artery which in turn is from the internal carotid artery. It leaves the orbit through the SON/SOF, divides into superficial and deep branches to supply the skin and muscles of the upper eyelid, forehead and scalp. The supraorbital vein unites with the supratrochlear vein near the medial angle of the eye to form the facial vein.8
The SON or SOF is considered to be reliably constant in their location. However, cosmetic surgeons are generally reluctant to perform brow lifts and other open, as well as endoscopic surgical procedures in this region for fear of injuring the supraorbital nerve and subsequent sensory loss.1,9,10 In our study, the SOF/SON measuring approximately 22 mm was observed from the midline, similar with the observations reported in other studies, where the distance between the SOF/SON and the midline was 20-30 mm.10,11 It is interesting to note that in one of the studies conducted on North Indian skulls; the average distance between the SOF/SON and the midline was 24 mm, which is slightly higher than the current observation. However, a much longer (29 mm) distance between the SOF and midline was observed in a study conducted on a Korean population,7 (Table 2).
There are reports of gender difference in the location of SOF and is considered to be of forensic importance. It has also been observed that the left supraorbital foramen is situated closer to the midline in females compared with males.12,20 The mean distance between the SOF/SON and the frontozygomatic suture was 29.34 mm on the right side and 28.7 mm on left side. Though most of the previous studies have measured the SOF/SON from the nasal midline; it can be difficult to accurately locate on the skin during surgery. Hence, measuring the distance between the SOF/SON and the frontozygomatic suture is considered to be a more reliable parameter, which was used in the current study. This parameter is easily measurable compared to the parameter used in many previous studies, namely; the distance between the SOF/SON and temporal crest.1,3,13
Table 2: Compilation of the different measurements of SOF /SON as reported by the previous studies.
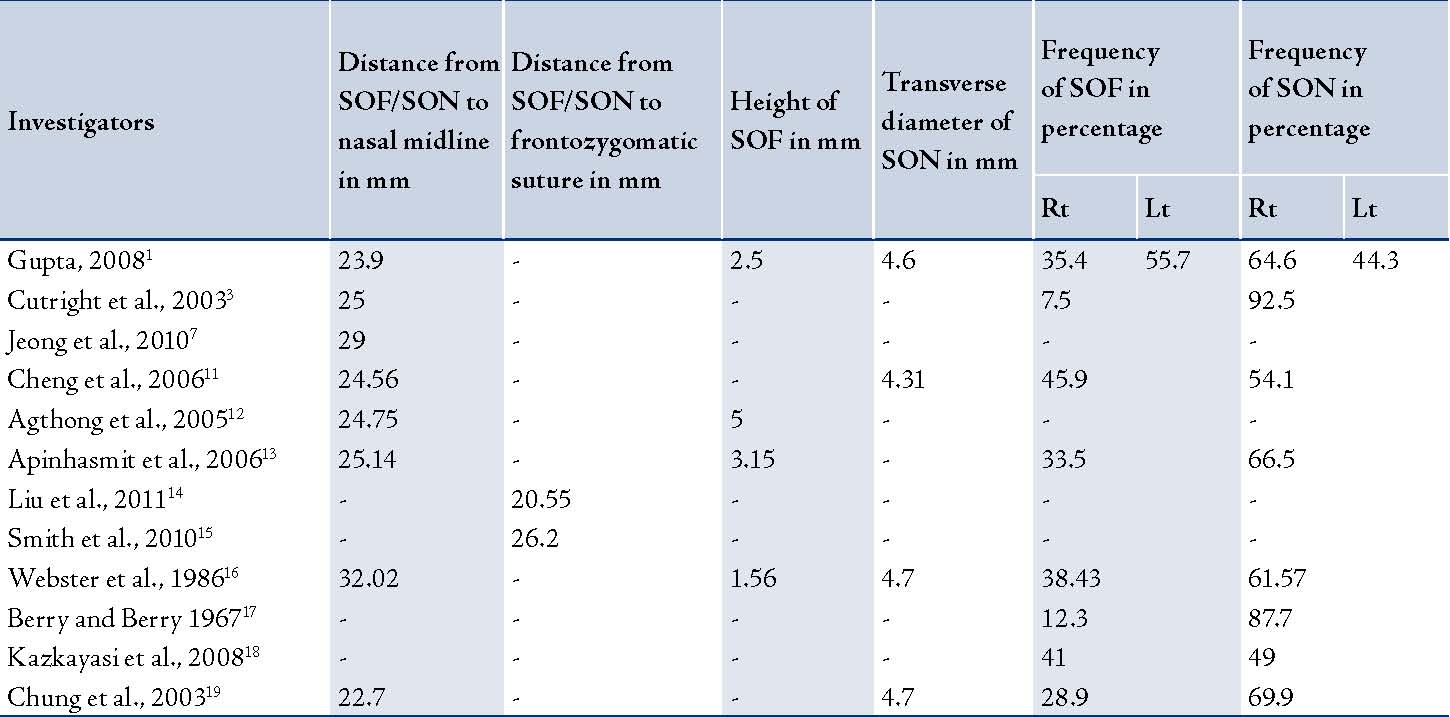
(SOF- supraorbital foramen; SON- supraorbital notch; Rt.- Right side; Lt.- Left side)
The frontozygomatic suture is easily palpable on the skin at a notch along the lateral orbital margin at the level of the lateral end of palpebral fissure.21,22 Hence, it becomes convenient for the surgeons to locate the SOF/SON from this point (frontozygomatic suture) compared to the temporal crest, which is not a point but rather a relatively elongated landmark. Few reports are available on the distance between the frontozygomatic suture and the SOF where the distance is reported to be less than the distance reported in the present study.14,15
Only a few available reports focus on the height and transverse diameter of SOF/SON. In the current study, we found that the mean height of SOF from the supraorbital margin was 3.5 mm on the right side and 3 mm on the left side; while the mean transverse diameter of SON was 5.17 mm on the right side and 5.58 mm on the left side. Gupta reported only the width of the SOF/SON in her study, which was 4.8 mm on the right side and 4.5 mm on the left side; which is approximately 1 mm less than the current observations.1 A study on Thai skulls has also revealed similar results, where they observed the SOF to be 2.81 mm and the SON 4.31 mm wide.11 Webster et al. have reported the height of SOF as 2.02 mm, width of the SON as 5.7 mm and the width of the SOF as 3.78 mm,16 (Table 2). The size of the SOF/SON may reflect the thickness of the supraorbital nerve and the caliber of the supraorbital vessels. It has been observed that the supraorbital notches which were less than 5 mm in width showed at least one accessory foramen indicating the early division of the supraorbital nerve and their exit through the accessory foramina.
There is a wide range of reports available regarding the frequency of the supraorbital foramen and supraorbital notch. Generally, the notches are considered to be more frequent than the foramina.23 In the present study, the SON was observed in 69.87% of cases and the SOF was observed in 28.91% of cases. A study conducted on Indian skulls also showed similar results where SON were more frequent compared to the SOF.16 Similarly, an earlier study conducted by Berry and Berry also reported markedly low frequency of SOF (12.3%) in North Indian skulls.17 However, a recent study conducted on a North-West Indian population has revealed a much balanced frequency of SOF and SON, which was 45.6% of SOF and 54.4% of SON.1 An almost equal ratio of SOF (41%) and SON (49%) was observed by Kazkayasi et al.18 They also found 10% of cases with the groove. The frequency of SOF was reported to be more in North East Asians and North American populations from an arctic region than the other populations.11,24
In another cross racial study, the frequency of SOF ranged from 8% to 51% depending upon the study population; it was lowest in a Burmese population and highest in Mexican populations.25 Among the available reports, the highest frequency (92.5%) of SON was observed by Cutright et al. in a study conducted on 40 black and 40 white cadaveric heads.3 An observation similar to the present study was made by Chung et al. in a study conducted on 124 Korean skulls, where they reported 69.9% cases of SON and 28.9% cases of SOF.19 According to Cheng et al. the supraorbital neurovascular bundle is relatively fixed in position in the supraorbital foramen,11 (Table 2). Hence, the neurovascular bundle is in great danger during surgical dissection; since during retraction, it is more likely to be stretched. Surgeons must take additional precautions during the reflection of scalp flaps in populations with a higher incidence of supraorbital foramina. It is evident by these reports that while performing forehead, coronal, brow or temple lift surgeries; palpating SON alone is not sufficient in locating the supraorbital neurovascular bundle. Therefore, surgeons should also be aware of the frequency of occurrence of SOF and their location well above the supraorbital margin.16
The occurrence of accessory supraorbital foramina is very common and is well documented. In our study, small additional openings medial, superior and lateral to the SOF/SON were observed in 66.25% of cases. This is relatively on the high side, compared to that of North West Indian population which was approximately 14%.1 Among other reports, Saylam et al. have found them in 21.2% of cases and Berry observed them in 50% of cases.4,25 As far as location of these accessory foramina is concerned, a majority of them (62.22% on the right side and 50% on left side) were found lateral to the SOF/SON. A similar observation was made by Gupta, who observed 84.6% of them lateral to the SOF/SON.1 However, Saylam et al. and Cheng et al. have observed most of the accessory foramina medial to the SOF/SON.4,11 The accessory foramina transmit the minor twigs of the supraorbital nerve which arise within the orbit and are responsible for incomplete analgesia following the injection at the SOF/SON.
The accurate anatomical location of SOF/SON is vital for both diagnostic and surgical procedures in this region. In recent years, the forehead, coronal, temple, brow lifting (blepharoplasty) and endoscopic procedures have gained impetus as substantial components of management of the aging face. Proper knowledge of forehead anatomy, especially of the supraorbital region is essential for those performing such cosmetic surgeries.16 The injury of supraorbital vessels and nerve may lead to complications such as: hematoma formation in the subgaleal plane; anesthesia or hypoesthesia of the forehead; and ischemia or necrosis of parts of the forehead flap and hair loss.16 Thorough knowledge of the SOF/SON and supraorbital neurovascular bundle is also important during procedures involving the superior orbital wall such as: frontal sinus obliteration; orbital decompression; botox injections; and exploration for the fractures and orbital exenteration. During these procedures, the SOF/SON are used as the reference points for the measurements of the superior orbital wall as they are found constantly close to the superior orbital margin.26 Irritation, entrapment and/or compression of the supraorbital nerve have been considered as frontal triggers of migraine headaches.27,28 Corrugator supercilii muscle resection is considered in such patients. Additionally, during corrugator resection; proper knowledge of anatomy of point of bony origin of the supraorbital nerve, its course and branches is vital for the surgeons.29
Conclusion
Overall, it can be stated that the position of the SOF/SON is not constant and it varies between different races and people of different regions. SON is observed more frequently compared to the SOF, though there is a slight difference in the frequency rate among the studies conducted in different regions and race groups. The occurrence of accessory supraorbital foramina is very common and is more frequently seen lateral to the main SOF/SON. Because of these variations of the exit point(s) of the supraorbital nerve and its branches; all the surgical procedures involving the supraorbital rim and adjoining areas have to be performed very carefully with the awareness of probable variations.
Acknowledgements
The authors declared no conflict of interest and no funding was received for this work.
References
1. Gupta T. Localization of important facial foramina encountered in maxillo-facial surgery. Clin Anat 2008 Oct;21(7):633-640.
2. Pareja JA, Caminero AB. Supraorbital neuralgia. Curr Pain Headache Rep 2006 Aug;10(4):302-305.
3. Cutright B, Quillopa N, Schubert W. An anthropometric analysis of the key foramina for maxillofacial surgery. J Oral Maxillofac Surg 2003 Mar;61(3):354-357.
4. Saylam C, Ozer MA, Ozek C, Gurler T. Anatomical variations of the frontal and supraorbital transcranial passages. J Craniofac Surg 2003 Jan;14(1):10-12.
5. Caputi CA, Firetto V. Therapeutic blockade of greater occipital and supraorbital nerves in migraine patients. Headache 1997 Mar;37(3):174-179.
6. Beer GM, Putz R, Mager K, Schumacher M, Keil W. Variations of the frontal exit of the supraorbital nerve: an anatomic study. Plast Reconstr Surg 1998 Aug;102(2):334-341.
7. Jeong SM, Park KJ, Kang SH, Shin HW, Kim H, Lee HK, et al. Anatomical consideration of the anterior and lateral cutaneous nerves in the scalp. J Korean Med Sci 2010 Apr;25(4):517-522.
8. Standring S, Ellis H, Healy JC, Johnson D, Williams A, Collins P, et al, eds. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 39th Edition, Elsevier, Churchill Liwingstone, London. 2005: 511-513.
9. Rosenberg GJ. The subperiosteal endoscopic laser forehead (SELF) lift. Plast Reconstr Surg 1998 Aug;102(2):493-501.
10. Erdogmus S, Govsa F. Anatomy of the supraorbital region and the evaluation of it for the reconstruction of facial defects. J Craniofac Surg 2007 Jan;18(1):104-112.
11. Cheng AC, Yuen HK, Lucas PW, Lam DS, So KF. Characterization and localization of the supraorbital and frontal exits of the supraorbital nerve in Chinese: an anatomic study. Ophthal Plast Reconstr Surg 2006 May-Jun;22(3):209-213.
12. Agthong S, Huanmanop T, Chentanez V. Anatomical variations of the supraorbital, infraorbital, and mental foramina related to gender and side. J Oral Maxillofac Surg 2005 Jun;63(6):800-804.
13. Apinhasmit W, Chompoopong S, Methathrathip D, Sansuk R, Phetphunphiphat W. Supraorbital Notch/Foramen, Infraorbital Foramen and Mental Foramen in Thais: anthropometric measurements and surgical relevance. J Med Assoc Thai 2006 May;89(5):675-682.
14. Liu DN, Guo JL, Luo Q, Tian Y, Xia CL, Li YQ, et al. Location of supraorbital foramen/notch and infraorbital foramen with reference to soft- and hard-tissue landmarks. J Craniofac Surg 2011 Jan;22(1):293-296.
15. Smith JD, Surek CC, Cortez EA. Withdrawn. Localization of the supraorbital, infraorbital, and mental foramina using palpable, bony landmarks. Clin Anat 2010 May;23(4):495.
16. Webster RC, Gaunt JM, Hamdan US, Fuleihan NS, Giandello PR, Smith RC. Supraorbital and supratrochlear notches and foramina: anatomical variations and surgical relevance. Laryngoscope 1986 Mar;96(3):311-315.
17. Carolineberry A, Berry RJ. Epigenetic variation in the human cranium. J Anat 1967 Apr;101(Pt 2):361-379.
18. Kazkayasi M, Batay F, Bademci G, Bengi O, Tekdemir I. The morphometric and cephalometric study of anterior cranial landmarks for surgery. Minim Invasive Neurosurg 2008 Feb;51(1):21-25.
19. Chung MS, Kim HJ, Kang HS, Chung IH. Locational relationship of the supraorbital notch or foramen and infraorbital and mental foramina in Koreans. Acta Anat (Basel) 1995;154(2):162-166.
20. Chrcanovic BR, Abreu MH, Custódio AL. A morphometric analysis of supraorbital and infraorbital foramina relative to surgical landmarks. Surg Radiol Anat 2011 May;33(4):329-335.
21. Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, Healy JC, et al, eds. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 40th Edition, Elsevier, Churchill Liwingstone, London. 2008: 409.
22. Tubbs RS, Loukas M, Shoja MM, Cohen-Gadol AA. Refined and simplified surgical landmarks for the MacCarty keyhole and orbitozygomatic craniotomy. Neurosurgery 2010 Jun;66(6)(Suppl Operative):230-233.
23. Turhan-Haktanir N, Ayçiçek A, Haktanir A, Demir Y. Variations of supraorbital foramina in living subjects evaluated with multidetector computed tomography. Head Neck 2008 Sep;30(9):1211-1215.
24. Hanihara T, Ishida H. Frequency variations of discrete cranial traits in major human populations. IV. Vessel and nerve related variations. J Anat 2001 Sep;199(Pt 3):273-287.
25. Berry AC. Factors affecting the incidence of non-metrical skeletal variants. J Anat 1975 Dec;120(Pt 3):519-535.
26. Huanmanop T, Agthong S, Chentanez V. Surgical anatomy of fissures and foramina in the orbits of Thai adults. J Med Assoc Thai 2007 Nov;90(11):2383-2391.
27. Guyuron B, Varghai A, Michelow BJ, Thomas T, Davis J. Corrugator supercilii muscle resection and migraine headaches. Plast Reconstr Surg 2000 Aug;106(2):429-434, discussion 435-437.
28. Guyuron B, Kriegler JS, Davis J, Amini SB. Comprehensive surgical treatment of migraine headaches. Plast Reconstr Surg 2005 Jan;115(1):1-9.
29. Janis JE, Ghavami A, Lemmon JA, Leedy JE, Guyuron B. The anatomy of the corrugator supercilii muscle: part II. Supraorbital nerve branching patterns. Plast Reconstr Surg 2008 Jan;121(1):233-240.
|