|
Introduction
Fine needle aspiration cytology (FNAC/FNA) has played a pivotal role in diagnosing thyroid gland nodules and thus pulling investigations out of the laboratory into the outpatient department. But in this procedure, the pitfalls encountered were either due to less pressure, inadequate specimen or due to excess pressure; the cells are flushed away with blood. A growing technique for thyroid nodules, fine needle capillary cytology (FNCC/FNC) bears hope of being a more efficient clinical investigation. It is the technique of using the same fine needle without the negative pressure as done in FNAC. The studies have shown that the two techniques have unique results in different areas, the sensitivity depends on whether the tumor is vascular, necrotic or other factors.1,2 In cases of thyroid lesions, promising results are encountered in favor of fine needle capillary cytology.1,3
Fine Needle Non Aspiration Cytology (FNCC), is a technique similar to FNAC which eliminates the need for aspiration by a syringe.4 It is less painful, less traumatic and allows for much better control of the needle while in the lesion. FNA when performed in vascular organs like the thyroid and vascular tumors results in hemorrhagic distortion of cell morphology in the aspirate. This hampers the study and diagnosis of the lesion thereby changing the course of management.5 This problem is overcome by the FNCC technique, which picks up a small amount of tissue in which the cell morphology and architecture is preserved. The advantages of FNCC are as follows: (a) it yields more material, (b) no hospitalization required for the procedure and (c) results are obtained rapidly within hours. However, the disadvantages are: (a) it compromises on cell concentration, (b) detrimental to cell morphology and active aspiration of blood, and (c) it relies heavily on the skill of the performer.4
FNC was developed in France by Brifford, Gentile and Hebert in 1982.6 It avoids aspiration and relies on the physical property of capillary pressure to suck cells inside the needle bore. The French authors termed the technique “Cytopuncture.” For thyroid lesions, this technique was first evaluated and compared with the conventional technique of FNA by Santos and Leiman.3 Many studies have proved that FNCC seemed to be better for diagnosing malignant lesions while FNA appeared better for diagnosing benign lesions.7,8,9,10,11 They opined that FNCC was more patient friendly, gave more cellular yield and that it will improve the quantity and quality of the material. Both the techniques should be used together yielding better diagnostic results.
With this idea in mind, the FNC technique can be used as a simple outpatient procedure in thyroid nodules. This study aims to compare the two cytopuncture techniques in our clinical set up to promote accurate diagnosis and better management.
Methods
This was a prospective study comparing FNC and FNA on 50 patients with a thyroid swelling/nodule who were admitted to Fr. Muller Medical College Hospital, Karnataka, India, over a period of 2 years from May 2006 to April 2008. The ethical committee clearance was obtained and all biopsies were performed by the same investigator. The Pathologist was blinded for the technique used and all cytological and histopathological reporting was done by a single pathologist. Histopathological specimen was available in 38 cases. The inclusion criteria comprised of all the patients admitted to the hospital with thyroid nodules or swellings (diagnosed by palpation) and patients aged >15 years. The exclusion criteria consisted of patients who had undergone previous surgery and patients who had undergone previous irradiation.
After detailed clinical examination along with ensuring to note any doubtful sites on the thyroid gland, the patient was investigated with a thyroid function test and a needle biopsy. The patient was subjected to needle biopsies (not ultrasound guided) after obtaining informed consent. The order of FNC and FNA sampling was pre-planned; in 25 patients, FNC was performed first followed by FNA and the next 25 patients underwent FNA first followed by FNC. This was done to eliminate any bias (if present). Both techniques were performed at the same site by the same investigator. A 23G needle was used in both procedures, and an average of 4 slides was obtained by both the FNA and the FNC techniques.
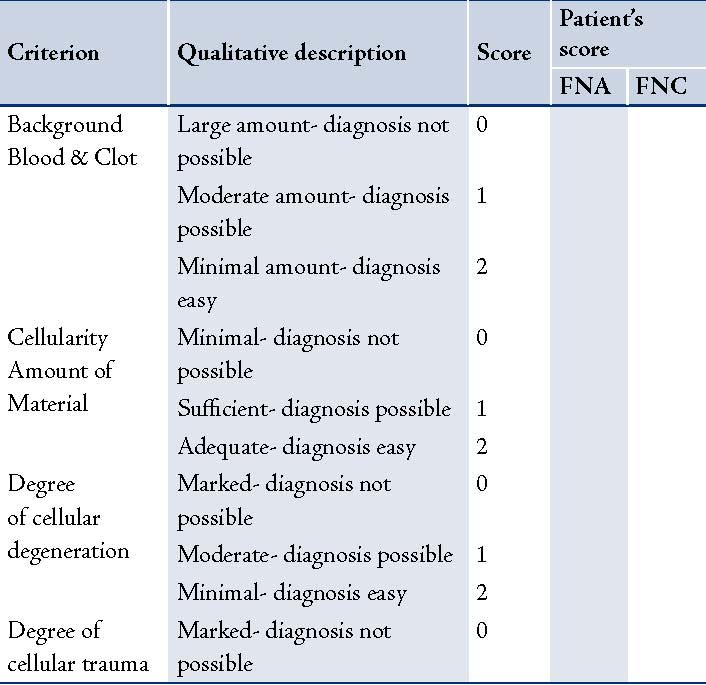
Some of the smears were fixed in methanol and stained by Papanicolaou stain, the others were air dried and stained using the May-Grunwald-Geimsa stain. The smears of FNC and FNA were assessed by a single observer using a scoring system (modified scoring system of Mair and colleagues, (Table 1).11 FNC and FNA results were correlated with histopathological findings whenever surgical specimens (38 cases) were available. The tissue was processed routinely and paraffin embedded blocks was prepared. Sections cut at 4-6 µm were stained with Hematoxylin and Eosin. The data collected was statistically analyzed and compared using the Receiver Operating Curve (ROC). The sensitivity, specificity and accuracy of both FNC and FNA were calculated. Sensitivity was defined as the ratio of true positives to the total number of patients with the disease; while specificity was defined as the ratio of true negatives to the total number of patients without the disease. Accuracy was defined as the ratio of true positives plus true negatives to the total number of patients.
The smears of FNC and FNA were assessed by a single observer using a scoring system which was a modified scoring system of Mair and colleagues.12 It was based on the following: 1) Background blood or clot, 2) Amount of cellular material, 3) Degree of cellular degeneration, 4) Degree of cellular trauma, and 5) Retention of appropriate architecture. A score ranging from 0-2 was assigned to each of these criteria. A cumulative score between 0-10 points was allocated to each FNC and FNA specimen which was then assigned to one of the three categories based on total points scored.
Unsuitable for cytodiagnosis 0 - 2
Diagnostically adequate 3 - 6
Diagnostically superior 7 - 10
Unsuitable specimen mainly contained blood clots or low cellularity leading to inadequacy in diagnosis. Diagnostically adequate specimen was good enough to give a diagnosis and exhibited moderate cellularity which was sometimes trapped in blood clots. Diagnostically superior were those specimens in whom the cellularity was good, the architecture was not destroyed with the least amount of blood clots.
The data collected was statistically analyzed and compared using the Receiver Operating Curve (ROC). Each parameter was analyzed and plotted as a line diagram where FNC was compared to FNA. Hence, the straight line in the graph represents FNA while the curved line represents FNC. The area below the FNC curve is calculated and depending on the area, it is comparable to FNA as follows:
Area below the curve Comparison
0.9 - 1.0 Excellent
0.8 - 0.9 Very Good
0.7 - 0.8 Good
0.6 - 0.7 Average
0.5 - 0.6 Poor
With the overall scores and the diagnostic description, FNC was correlated to FNA using the Kappa score.
<0.20 - Poor agreement
0.21 - 0.4 - Fair agreement
0.41 - 0.6 - Moderate agreement
0.61 - 0.8 - Good agreement
0.81 - 1.0 - Very good agreement
Table 1: Scoring system developed by Mair et al.7,12
Results
In this study, the majority of the patients were aged between 40 and 49 years (36%), with a mean age of 39.16 (SD 11.47; Table 2). In this study, females comprised 94% of the study group, while males comprised only 6%. Thyroid function tests of all the patients were within normal limits, except for one patient who had elevated T-3 and T-4 values.
Table 2: Age Distribution.
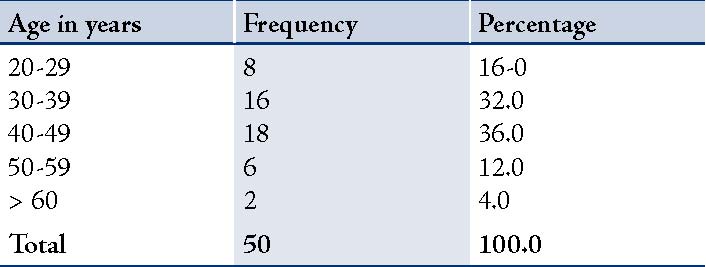
(SD-11.472; range: 20-72)
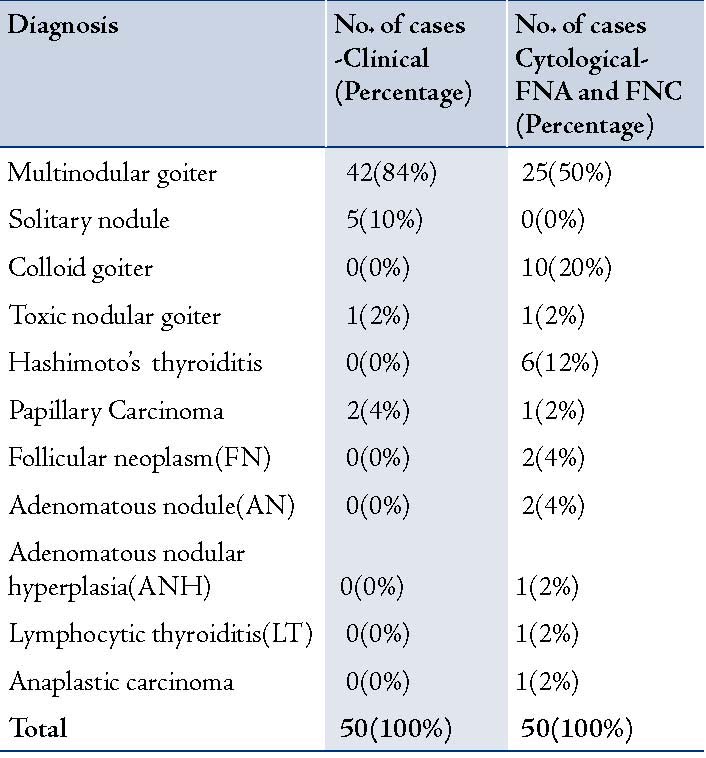
Clinically, 42 of the 50 cases were multi-nodular goiters, 5 were solitary nodules, 1 was a toxic nodular goiter and 2 were suspicious of malignancy. The cytological evaluation diagnosed 25 (50%) cases of nodular goiters, 10 (20%) cases of colloid goiters, 6 (12%) cases of Hashimoto’s thyroiditis and 1 case (2%) each of anaplastic carcinoma and papillary thyroid carcinoma. (Table 3)
Table 3: Correlation between clinical diagnosis with FNAC and FNCC.
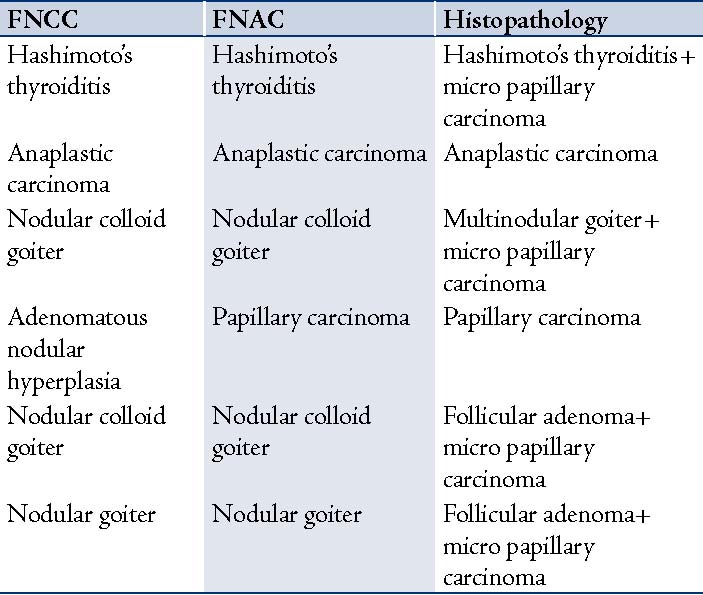
A comparison between FNCC and FNAC is shown in Table 4. Of the 50 patients in the current study, six were diagnosed to have thyroid malignancy on final histopathology report. Four patients were not diagnosed by FNC nor FNA needle sampling but only on histopathology. All the four had microscopic foci of papillary carcinoma. The specimen of anaplastic carcinoma had typical characteristics in FNC and the FNA smears both were equally scored. The papillary carcinoma was diagnosed only with FNA since the FNC specimen was inadequate in material. But the one specimen which was diagnosed as anaplastic carcinoma, the FNC specimen was good and better than FNA with respect to the amount of cellularity and retention of architecture.
Table 4: Comparison between FNCC and FNAC diagnosis.
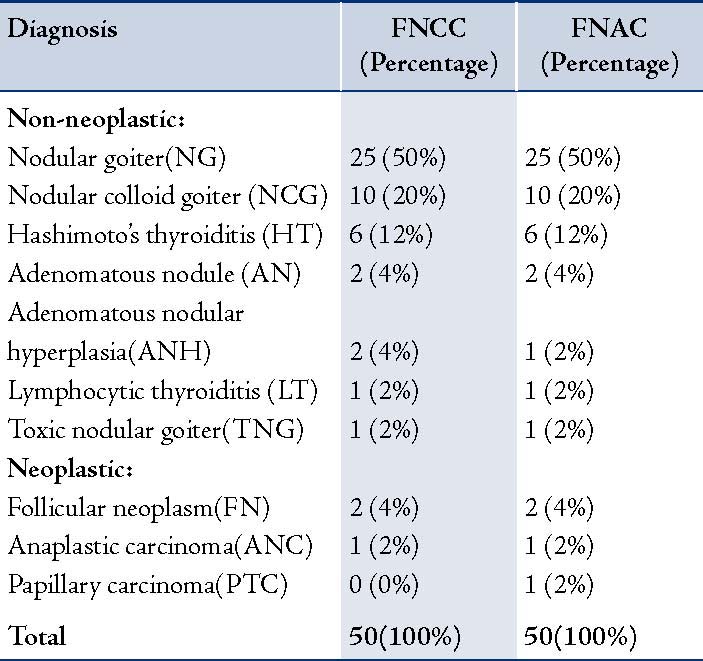
Table 5: Comparison of FNCC and FNAC with Histopathology report of 38 cases.
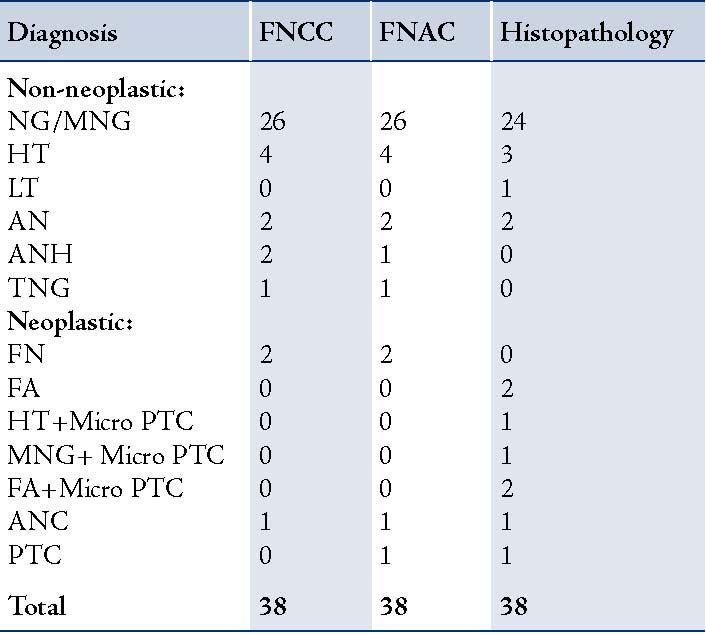
Histopathological specimen were obtained in 38 cases which were correlated with both the needle biopsies (Table 5). Four patients exhibited microscopic focus of malignancy incidentally diagnosed on final histopathology. These cases could not be diagnosed on FNCC or FNAC. (Table 6)
Table 6: Correlation of FNCC and FNAC with histopathology report in six cases of malignancy.
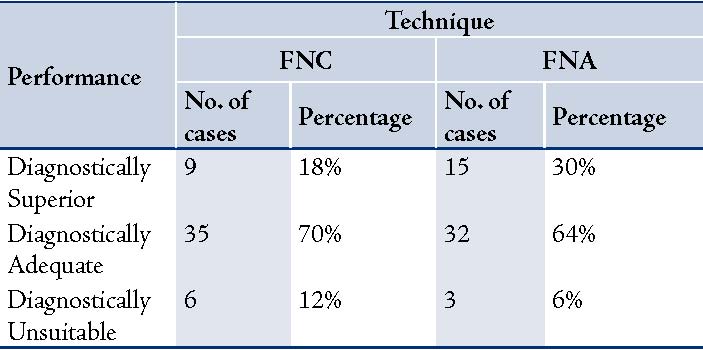
The diagnostic performance of FNC and FNA techniques indicated that FNA yielded more diagnostically superior cases (30%) compared to FNC (18%). But FNC produced more cases that were adequate for diagnosis (70%) than FNA (64%). Moreover, FNA exhibited half the number of diagnostically unsuitable cases (6%) compared to FNC (12% [Table 7]). The kappa value was 0.29, which was a fair agreement between the two techniques.
Table 7: Diagnostic performance.
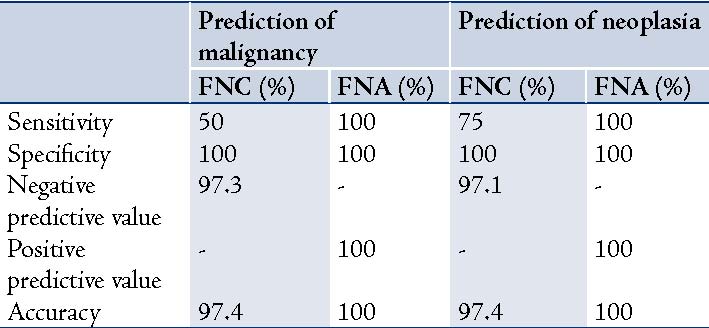
FNC showed 50% sensitivity and FNA showed 100%, while specificity was 100% for both the techniques; but the accuracy score was 97.4% for FNC and 100% for FNA for predicting malignancy. While for predicting neoplasia; sensitivity was 75% for FNC and 100% for FNA, specificity was 100% for both the techniques, while the accuracy score was 97.4% for FNC and 100% for FNA. (Table 8)
Table 8: Prediction of malignancy and neoplasia.
Discussion
Thyroid disorders vary in terms of their presentation and characteristics. An established first line of investigation for any evident thyroid swelling is a Fine Needle Aspiration Cytology (FNAC) after a thyroid function test.4 It has gained popularity based on the given facts.4 It is easy and quick to perform, and has a high degree of sensitivity and specificity. In the current study, the FNC and FNA techniques were compared on thyroid gland lesions using a modified scoring system by Mair et al.12 The age incidence of thyroid gland disorders was between 40-49 years, which mainly comprises middle aged patients. This has previously been stated in literature and has also been observed by other authors.1,3,13,14 Our study group was comprised of 94% female patients and 6% males; none of the male showed malignant disease.
In comparing both techniques on the parameter of blood clots; FNC was most likely to produce the least likelihood of hemorrhage, thereby giving a clear picture to the cytopathologist. This has also observed by Ali Rizvi,1 and other authors.3,14 The presence of blood cannot be totally prevented in thyroid gland cytology samples but its effect can be minimized by the capillary action of the FNC technique compared to the active high suction pressure of the FNA technique. In our study, for material with highly cellular lesions in which abundant material was obtained; FNC was more likely to be diagnostically superior; but FNA can diagnose most of the lesions. In less cellular lesions, FNA is more likely to be diagnostically superior to FNC. Some authors have reported similar findings,10,12 but the majority found no significant difference.3,11,12,13
The cellular trauma and degeneration were generally the same in both techniques as these parameters depended on the method of smear making. FNA scored better since it had more cellular material, hence the destruction of some sheets of cells did not obscure the field for diagnosis. This is in contrast to Raghuveer et al. who opined FNC smears were better.11 The architecture was retained to a greater extent in the FNA smears than the FNC smears due to the additional material yield in FNA. But the architecture was a text book picture in whichever FNC smears that had good material. Gosh and Misra observed this in their study of FNC on thyroid lesions.15 This was the only parameter in which FNC scored much better than FNA, as reported by other authors.3,11,14
Three patients were diagnosed to have thyroid cysts; in two of these patients, FNC was performed first and a colloid overflow was encountered, it was drained using the FNA technique. There was no cellular material on any of these smears; hence they was not included into the study. This problem has also been previously encountered by Mair and team,12 and also by Kate et al.16 They documented that FNA is the procedure of choice for cystic lesions, as the fluid can be collected for cytological evaluation. The cysts usually disappear after the colloid is drained out completely; hence FNA becomes a therapeutic procedure. The specimen of anaplastic carcinoma had typical characteristics in FNC and the FNA smears, both were equally scored.
The papillary carcinoma was diagnosed only with FNA as the FNC specimen was inadequate in material. Hence in contradiction to the analyses by Santos and Leiman who stated that FNC specimen were better in neoplasms; we encountered some technical difficulty in assessing the quality of the FNC specimen in malignancies.3 But in the one specimen which was diagnosed as anaplastic carcinoma, the FNC specimen was relatively good and generally better than FNA with respect to the amount of cellularity and retention of architecture.
On the diagnostic performance; FNA was notably better, producing more of the diagnostically superior specimen (n=15; 30%), compared to FNC (n=9; 18%); however, FNC exhibited more diagnostically adequate specimen (n=35; 70%). Santos and Leiman reported similar results which were 44% diagnostically superior, 50% diagnostically adequate and 3% diagnostically unsuitable with the FNC technique.3 Rizvi and Hussain also reported that FNC yielded 44.7% diagnostically superior specimen, 53.3% diagnostically adequate and 2% diagnostically unsuitable specimen.1
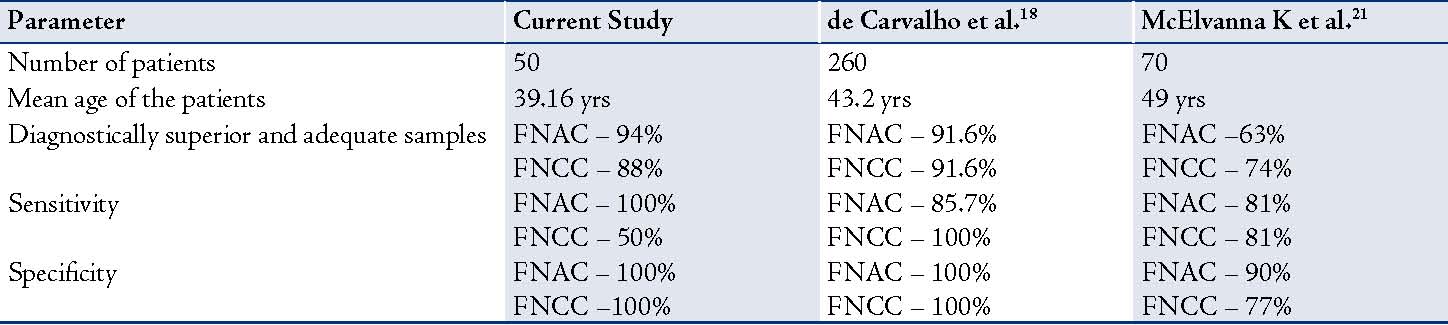
In this study, FNC appears to be a good technique but only in certain aspects compared to FNA. Each of these techniques has its own advantages and disadvantages.4 Sanjeev et al. conducted a similar study on lymph node lesions and the results proved the technical superiority of FNCC technique in cellular lymph node lesions.17 While Carvalho et al. suggested that FNA and FNC provide similar sample adequacy and diagnostic accuracy.18 Overall, the decision to chose which technique to adopt rests with the operator to select the method that will produce a high yield of good quality material, with minimal diagnostic failures. Though there was no significant difference between the two techniques, if done in tandem at two different sites on the same lesion; they can add up to ease the diagnosis.19,20 The results of this study were compared to those reported by Carvalho et al.18 and McElvanna et al.21 who have also documented similar observations. (Table 9)
Table 9: Comparison of the current study with other studies.
Conclusion
In summary, both techniques FNC and FNA are advised to be used in tandem; however, they should be done on different sites of the same thyroid lesion. Preferably, FNC should be performed initially, and then followed by FNA in order to attain clear and accurate cytological diagnosis. In highly cellular lesions where abundant material was obtained, FNC was most likely to be diagnostically superior, although FNA can also diagnose most of the lesions. In less cellular lesions, however; FNA was most likely to be diagnostically superior to FNC.
Acknowledgements
The authors reported no conflict of interest and no funding was received on this work.
References
1. Rizvi SA, Husain M, Khan S, Mohsin M. A comparative study of fine needle aspiration cytology versus non-aspiration technique in thyroid lesions. Surgeon 2005 Aug;3(4):273-276.
2. Braun H, Walch C, Beham A, Moinfar F. Fine needle capillary cytology versus fine needle aspiration cytology–a comparison of quality between puncture techniques in the ENT area. Laryngorhinootologie 1997 Jun;76(6):358-363.
3. Santos JE, Leiman G. Nonaspiration fine needle cytology. Application of a new technique to nodular thyroid disease. Acta Cytol 1988 May-Jun;32(3):353-356.
4. Orrel SR, Gregory F. Sterrett, Whitaker D, Fine Needle Aspiration Cytology, 4th ed, New Delhi, Elsevier, 2005; pg 125-64.
5. Dey P, Ray R. Comparison of fine needle sampling by capillary action and fine needle aspiration. Cytopathology 1993;4(5):299-303.
6. Briffod M, Gentile A, Hébert H. Cytopuncture in the follow-up of breast carcinoma. Acta Cytol 1982 Mar-Apr;26(2):195-200.
7. Pothier DD, Narula AA. Should we apply suction during fine needle cytology of thyroid lesions? A systematic review and meta-analysis. Ann R Coll Surg Engl 2006 Nov;88(7):643-645.
8. Suen KC, Quenville NF. Fine needle aspiration biopsy of the thyroid gland: a study of 304 cases. J Clin Pathol 1983 Sep;36(9):1036-1045.
9. Jayaram N, Chetan M, Prasad SR, Ramaprasad AV. Thyroiditis: Thyroid Function and Cytologic Correlation- A study of 66 cases. Journal of Cytology 1996;13:21-24.
10. Kamal MM, Arjune DG, Kulkarni HR. Comparative study of fine needle aspiration and fine needle capillary sampling of thyroid lesions. Acta Cytol 2002 Jan-Feb;46(1):30-34.
11. Raghuveer CV, Leekha I, Pai MR, Adhikari P. Fine Needle Aspiration cytology versus Fine Needle Sampling without aspiration. A prospective study of 200 cases. Indian J Med Sci 2002 Sep;56(9):431-439.
12. Mair S, Dunbar F, Becker PJ, Du Plessis W. Fine needle cytology–is aspiration suction necessary? A study of 100 masses in various sites. Acta Cytol 1989 Nov-Dec;33(6):809-813.
13. Jayaram G, Gupta B. Nonaspiration fine needle cytology in diffuse and nodular thyroid lesions: a study of 220 cases. Acta Cytol 1991 Nov-Dec;35(6):789-790.
14. Haddadi-Nezhad S, Larijani B, Tavangar SM, Nouraei SM. Comparison of fine-needle-nonaspiration with fine-needle-aspiration technique in the cytologic studies of thyroid nodules. Endocr Pathol 2003;14(4):369-373.
15. Ghosh A, Misra RK, Sharma SP, Singh HN, Chaturvedi AK. Aspiration vs nonaspiration technique of cytodiagnosis–a critical evaluation in 160 cases. Indian J Pathol Microbiol 2000 Apr;43(2):107-112.
16. Kate MS, Kamal MM, Bobhate SK, Kher AV. Evaluation of fine needle capillary sampling in superficial and deep-seated lesions. An analysis of 670 cases. Acta Cytol 1998 May-Jun;42(3):679-684.
17. Sajeev S, Siddaraju N. A comparative analysis of fine-needle capillary cytology vs. fine-needle aspiration cytology in superficial lymph node lesions. Diagn Cytopathol 2009 Nov;37(11):787-791.
18. de Carvalho GA, Paz-Filho G, Cavalcanti TC, Graf H. Adequacy and diagnostic accuracy of aspiration vs. capillary fine needle thyroid biopsies. Endocr Pathol 2009;20(4):204-208.
19. Ceresini G, Corcione L, Morganti S, Milli B, Bertone L, Prampolini R, et al. Ultrasound-guided fine-needle capillary biopsy of thyroid nodules, coupled with on-site cytologic review, improves results. Thyroid 2004 May;14(5):385-389.
20. Baksh S, Masih K, Singh S, Das S. Diagnostic utility of fine needle non-aspiration cytology versus fine needle aspiration cytology in breast masses. Indian J Pathol Microbiol 2004 Jul;47(3):319-321.
21. McElvanna K, Pyper PC, Miller K. A comparison of fine needle aspiration vs. non-aspiration cytology of thyroid nodules. Int J Surg 2010;25(2).
|