A 40-year-old Omani male presented with a history of recurrent mild dyspnea and chest discomfort of long duration. This was associated with occasional heaviness in the right thoracic region. He had no associated fever or cough during the attacks. However, the patient admitted a history of road traffic accident 14 years prior with a history of right lung trauma. On examination, he had decreased air entry in the right lower lobe but an otherwise normal examination. Chest X-ray revealed a mass in the right lower lobe. We subsequently performed a computed tomography (CT) scan [Figure 1a and b].

Figure 1: Selected (a) coronal and (b) sagittal contrast-enhanced computed tomography images of the chest and upper abdomen revealed a rounded homogenous mass lesion in the right thoracic cavity within the right lower lobe.
Question
- What is the most likely diagnosis?
a. Right lower lobe consolidation.
b. Right-sided diaphragmatic rupture with partial herniation of the liver through diaphragmatic defect.
c. Displacement of the right diaphragm and a ‘peak’ at the middle (juxtaphrenic peak).
d. A pleural mouse (also known as a fibrin body), a mobile rounded clump of fibrin left over after resolution of a pleural effusion.
e. Lobar form of bronchoalveolar cell carcinoma.
Answer
b. Right-sided diaphragmatic rupture with partial herniation of the liver through diaphragmatic defect.
Discussion
Our patient had a right-sided diaphragmatic rupture with partial herniation of the liver through diaphragmatic defect, which occurred post-trauma. In this condition, the small rounded mass of liver herniates into the right thoracic cavity, while the largest part of the liver remains in the abdominal cavity, an appearance which has been fancifully likened to a cottage loaf of bread. For that reason, the radiological appearance of this condition had been called the ‘cottage loaf sign’ [Figure 2a and b].
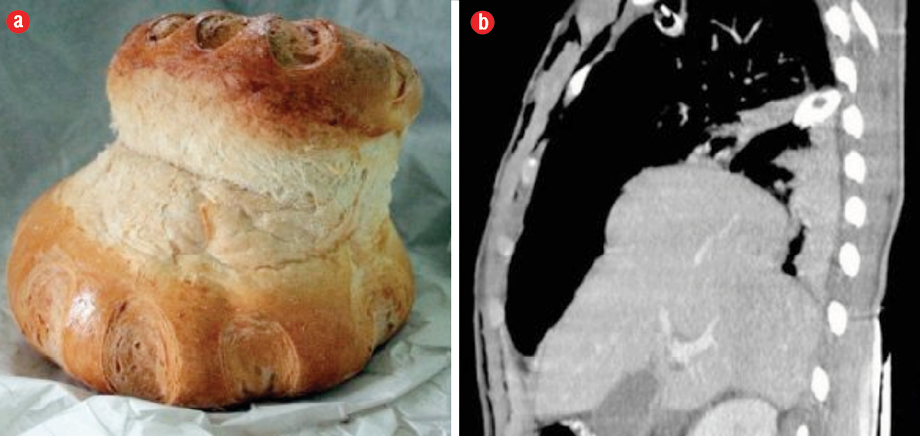
Figure 2: (a) Cottage loaf. (b) Cottage loaf sign as seen on computed tomography imaging.
Diaphragmatic rupture often occurs after blunt abdominal trauma, for example, after a motor vehicle accident. For that reason, it predominates in young males.
In patients who sustain lower thoracic or blunt abdominal trauma,1 the estimated incidence is ~4.5% (range = 0.8–8%). The most common reported herniated viscera are the colon and stomach. Due to the possible buffering effect of the liver, the left hemidiaphragm injury is noted three-times more frequently than the right. Most ruptures measured are longer than 10 cm and are found at the posterolateral aspect of the left hemidiaphragm.2
This condition is not recognized at the time of the trauma in most cases. Symptoms may take time to appear from the trauma onset and cases may be undiagnosed for months or even years if not recognized in the first 48 hours.
An accurate, noninvasive diagnostic technique is needed in this condition because blunt abdominal trauma is usually managed conservatively with the seldom need for exploratory laparotomy. CT is the main investigation of choice for those patients, most of whom undergo a whole-body CT examination.3
references
- Killeen KL, Mirvis SE, Shanmuganathan K. Helical CT of diaphragmatic rupture caused by blunt trauma. AJR Am J Roentgenol 1999 Dec;173(6):1611-1616.
- 2. Iochum S, Ludig T, Walter F, Sebbag H, Grosdidier G, Blum AG. Imaging of diaphragmatic injury: a diagnostic challenge. Radiographics 2002;22 Spec No:S103-S116; discussion S116-S118.
- 3. Desir A, Ghaye B. CT of blunt diaphragmatic rupture. Radiographics 2012 Mar-Apr;32(2):477-498.