Inferior vena cava (IVC) anomalies are uncommon. Duplicated IVC is the second most common anatomical anomaly of the IVC, with a prevalence of 1.5%.1 Most IVC anomalies are discovered incidentally during IVC filter placement consultation or radiological study performed for another purpose. Filter placement in a duplicated IVC has many options, including the suprarenal position or placing a filter in both IVCs. These options are proven to be safe and effective but depend on the preference of the interventionist and cost-effectiveness. There are few case reports of filter placement in the duplicated IVC. We report a case of duplicated IVC with filter placement in the suprarenal position.

Figure 1: (a) Coronal and (b) axial computed tomography images showing duplicated inferior vena cava (red arrows).
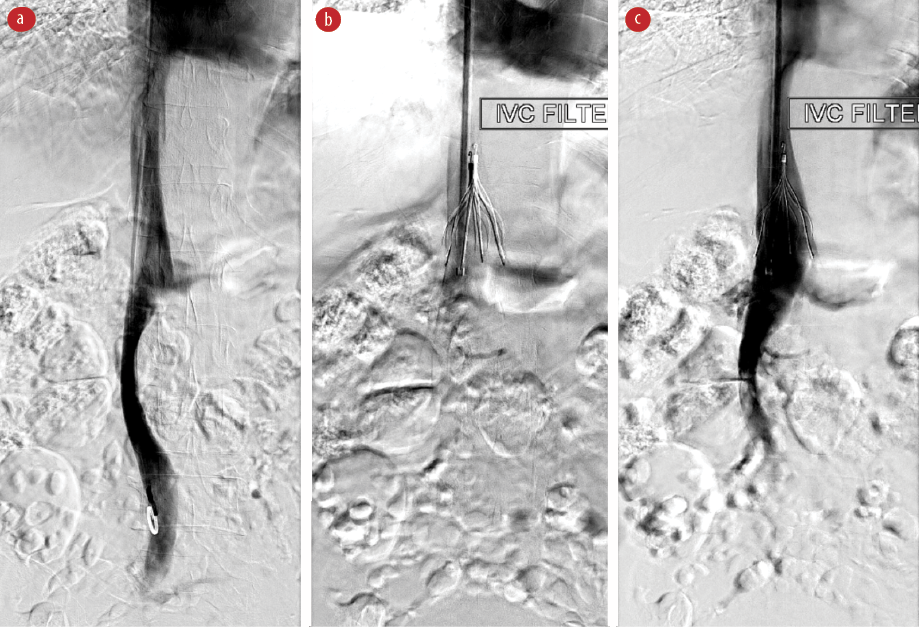
Figure 2: (a) Digital subtraction venogram performed by a pigtail catheter demonstrates duplicated IVC, (b) the pigtail catheter is in the right IVC, and (c) completion venogram of suprarenal placement of the
IVC filter.
Case report
Our patient was a 51-year-old female with hypertension and dermatomyositis with a recent significant pulmonary embolism event. She was also newly diagnosed with bladder cancer and planned for transurethral resection of the tumor. She was seen by a hematologist and was not a candidate for anticoagulation. An IVC filter placement was requested accordingly.
The patient was brought to the adiology department for IVC filter placement. Previous enhanced computed tomography was reviewed and showed double IVC [Figure 1]. Right jugular vein access approach was performed with ultrasound guidance, and a 7 Fr vascular sheath was inserted over a wire. A 5 Fr pigtail catheter was inserted and advanced to the lower IVC. Central venography was performed and confirmed duplicated IVC [Figure 2]. The IVC filter (Gunther Celect, Cook Medical) was placed in the suprarenal segment of the IVC.
The procedure was uneventful with no immediate procedure-related complications. Following the procedure, the patient was observed in the ward and was doing well. She underwent transurethral resection of the bladder tumor uneventfully. No signs of pulmonary thromboembolism developed following the IVC filter placement.
Discussion
A duplicated IVC occurs when the supracardinal veins persist bilaterally.2 This configuration is estimated to be present in 0.2–3% of the general population.3 With this anomaly, the iliac veins typically drain into the ipsilateral IVC.2 The IVCs vary greatly in size and may be symmetric, but a dominant IVC typically occurs, usually on the right side. This anomaly has multiple associations with cardiovascular and urinary system malformation.
Recognizing this rare vascular anomaly is very important before attempting any surgical or radiological intervention related to the IVC. One of these procedures is IVC filter placement.
Identification of duplication of the IVC is important in patient treatment because if the entity is not recognized before routine placement of an infrarenal IVC filter, recurrent pulmonary embolism can develop.4 Owing to the relative rarity of this anomaly, the approach to filter placement is largely debatable.2 The most often described approach is placement of IVC filters in the bilateral infrarenal IVCs; however, there are reports of placing an IVC filter in the common suprarenal IVC.2,5
Anatomically, the IVC is formed by the confluence of the right and left common iliac veins draining blood from the lower extremities and pelvis. As it ascends in the retroperitoneum to the right of the abdominal aorta, the IVC receives major tributaries, including the lumbar veins, the left and right renal veins, the right gonadal vein, and the hepatic veins. The azygos venous system connects to the IVC either directly or through the renal veins. The IVC and its branches are best seen in the coronal plane. Duplicated IVC commonly appears as a continuation of the left common iliac vein crossing anterior to the aorta at the renal vein level to join the right-sided IVC.3,5 The best imaging modality to evaluate the IVC is contrast-enhanced multidetector computed tomography.5,6
It is always recommended to review prior cross-sectional images before IVC filter placement. If no images are available, cavography should be performed through the left iliac vein. A filter can then be placed into each cava or at the suprarenal portion of
the IVC.
IVC filter is commonly performed to prevent pulmonary embolism in patients with hypercoagulable states or documented venous thromboembolic disease and contraindications to anticoagulant therapy. There are many types of IVC filters available in the market, which can be deployed by the femoral or jugular approach and can be used as retrievable or permanent filters. Ideally, IVC filters are placed below the renal veins. However, in cases of congenital anomalies of the IVC and its tributaries, alternative placement locations or additional filters must be considered to prevent embolization through accompanying pathways. Venography is routinely performed before filter placement to determine the level of the renal veins, allow measurement of IVC diameter, and detect IVC and renal vein anomalies. Clues to duplication of the IVC on venography include lack of visualization of the left iliac inflow and larger-than-expected left renal
vein inflow.1
Few cases of duplicated vena cava filter placement have been reported. Indications of filter placement in IVC in these cases were: contraindication to anticoagulation use, bleeding and recent neurosurgery, prevention of massive pulmonary thromboembolism in cases of extensive proximal deep venous thrombosis, and pulmonary thromboembolism in cases of anticoagulation.7 In these cases, the filters were implanted in different positions, including the suprarenal position, filters in both cava branches, or parallel to the
left branch.3,8
All these options of filter placement proved to be safe and adequate. The choice depends on interventionist preference, availability of materials, and cost-effectiveness. The suprarenal position is considered effective, safe, and easily approached.3,9 It is cost-effective as one filter is used, and additional procedures can be avoided, such as embolization of one of the vena cava or its interconnection. In our case, we elected to deploy a single filter at the suprarenal portion of the IVC.
Our patient remained asymptomatic after the procedure with no procedure-related complications. A few weeks after the surgery, the IVC filter was retrieved uneventfully.
Conclusion
Duplicated IVC is a rare vascular anomaly that needs to be identified before considering IVC filter placement. Prior cross-sectional imaging to study IVC anatomy is important and is regarded as a pre-procedure requirement in some centers before placing an IVC filter. A suprarenal IVC filter placement is a safe and effective option in cases of a duplicated IVC.
Disclosure
The authors declared no conflicts of interest. Informed patient consent of publication was obtained.
references
- 1. Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH Jr. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics 2000;20(3):639-652.
- 2. Doe C, Ryu RK. Anatomic and technical considerations: inferior vena cava filter placement. Semin Intervent Radiol 2016 Jun;33(2):88-92.
- 3. British committee for standards in haematology writing group, Baglin TP, Brush J, Streiff M. Guidelines on use of vena cava filters. Br J Hematol 2006;134(6):590-595.
- 4. Malgor RD, Sobreira ML, Boaventura PN, Moura R, Yoshida WB. Filter placement in duplicated inferior vena cava: case report and review of the literature. J Vasc Bras 2008;7(2):167-170.
- 5. Sheth S, Fishman EK. Imaging of the inferior vena cava with MDCT. AJR Am J Roentgenol 2007 Nov;189(5):1243-1251.
- 6. Sartori MT, Zampieri P, Andres AL, Prandoni P, Motta R, Miotto D. Double vena cava filter insertion in congenital duplicated inferior vena cava: a case report and literature review. Haematologica 2006;91(6 Suppl):ECR30.
- 7. Steven M. Zangan, MD, and Thuong G. Van Ha, MD, Applied Radiology, University of Chicago, Chicago. April 27;2012.
- 8. Anne N, Pallapothu R, Holmes R, Johnson MD. Inferior vena cava duplication and deep venous thrombosis: case report and review of literature. Ann Vasc Surg 2005;19(5):740-743.
- 9. Smillie RP, Shetty M, Boyer AC, Madrazo B, Jafri SZ. Imaging evaluation of the inferior vena cava. Radiographics 2015;35(2):578-592.