HIV infection remains a major global public health issue. Humans acquire it via the exchange of bodily fluids, mainly through unprotected intercourse, and women pass it on via mother-to-child transmission (MTCT) during pregnancy, childbirth, and breastfeeding. Other known means of transmission include the use of infected syringes by drug abusers and blood transfusions.1
According to a report issued by the World Health Organization (WHO) in 2019, approximately 38 million people were living with HIV globally.2 In 2016, the American Foundation for Aids Research census showed that 51% of all adults living with HIV were women, and it is believed to be the leading cause of death for women in the reproductive age group worldwide.3,4
In the absence of any intervention, MTCT ranges from 15%–45%.4 With advancements in healthcare, improved access to and availability of antiretroviral therapy (ART), there has been a 50% reduction in new HIV cases. Preventative strategies have reduced MTCT to < 5%.4
In Oman, the first notified case of AIDS was in 1984.5 Up to 2019, the total number of cases of HIV/AIDS registered with the Ministry of Health (MOH) was 3232. Of those, 884 (27.4%) were female, the majority of which were of childbearing age; 63.1% were between the ages of 25–49 years, and 17.6% aged 15–24 years.5 There has been an exponential increase in the number of documented HIV cases in recent years, and this has been attributed to the decrease in stigmatization, applying protocols of detection such as antenatal screening (ANS) of pregnant women and their contacts as well as the availability of treatment in health institutions.5 The most common mode of transmission to children is MTCT from HIV-infected woman.
Oman established the Maternal and Child Health Program in 1987, intending to identify and care for all pregnant women and their offspring. In 2009, HIV testing was made mandatory for all women attending antenatal clinics for early detection, support, management, and prevention of transmission. In a study conducted by the MOH between 2009 and 2014, the testing coverage for HIV in pregnant women was 98% with a prevalence of 0.02% and an annual rate of HIV in the newborn due to MTCT of 0.01% or 10 per 100 000 live births.6
In Sultan Qaboos University Hospital (SQUH), a study looked into HIV-1 and 2 among pregnant women over 10 years between January 1995 and December 2005 and found a prevalence of 0.13%.7 The study did not look into the outcomes of the patient or their offspring, and it did not give information on whether or not patients were on ART or their antenatal management.
Worldwide, studies have been done to look into the effects on pregnancy and outcomes. For example, a retrospective study published in 2015, looked into the maternal and perinatal outcomes of HIV-infected women in a tertiary care hospital in Nigeria. They concluded that HIV-positive status increased adverse birth outcomes of pregnancy such as anemia, puerperal sepsis, low birth weight, preterm births, and higher cesarean section rate amongst women who tested positive for HIV. It also showed that ART appeared to reduce the risk of preterm births in HIV-positive cohorts.8
On the contrary, a prospective observational study published in 2015 looked into antiretroviral therapy in relation to birth outcomes in Dar es Salaam, Tanzania. They not only compared the outcome of ART versus non-exposure to ART during pregnancy, but also the outcomes related to the ART therapy used (e.g., zidovudine monotherapy vs. highly active antiretroviral therapy (HAART)) and found that there was an increased risk of adverse birth outcomes associated with the use of HAART.9
We sought to investigate the prevalence of HIV in pregnant Omani women, and identify the maternal, obstetrical, and neonatal outcomes over 13 years (2005–2017) at SQUH, a tertiary hospital in Muscat, Oman.
Methods
This was a retrospective, descriptive, cross-sectional study of HIV-positive pregnant women that were managed and delivered in the department of obstetrics and gynecology (OBGYN) at SQUH. We set an unlimited sample size during the study period (1 January 2005 to 31 December 2017) due to the relatively low prevalence of the disease. We included all pregnant Omani women who tested positive for HIV-1 or 2 on ANS during this period. We excluded all non-Omani’s to get a true prevalence of HIV in the Omani population.
After obtaining ethical approval from the hospital’s ethics committee, we collected data from the hospital information system.
Our data collection sheet included a variety of variables, including initial demographics, past medical, surgical, and obstetrical history, and allergies. Each woman who tested positive was then divided by the number of pregnancies, and each pregnancy was considered a separate case.
Each case was then looked into further: whether or not HIV status was known during the pregnancy; the gestation at first presentation whether it was a single or multifetal pregnancy; the viral load and CD4 count per trimester; the use of ART; and the gestational age at which they have started treatment, compliance to medication, the outcome of pregnancy, mode of delivery, confounding obstetrical complications, antepartum complications, acquired antepartum opportunistic infections, intrapartum complications, whether or not they received intrapartum ART prophylaxis, and postpartum complications. We also looked at whether or not these patients were advised for or against breastfeeding.
Data collected regarding fetal outcomes included gestational age at delivery, birth weight, sex, Apgar scores, and whether or not they required neonatal intensive care unit (NICU) admission. Additionally, neonatal prophylactic ART, postnatal HIV status on testing, emergency visits, and outpatient department visits were explored.
Data were then transferred to EpiData. The information was analyzed using SPSS Statistics (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.) to calculate measures of central tendency and dispersion.
Results
A total of 104 281 ANS (number of pregnancies) were done over the study period. Excluding repeated pregnancies, this number dropped to 13 688, corresponding to the number of patients, to achieve prevalence.
Twenty-nine Omani pregnant women tested positive for HIV on ANS. Fourteen (48.3%) had proven positive for HIV after further testing with polymerase chain reaction. Therefore, the true prevalence of Omani pregnant women in SQUH who tested positive for HIV was 0.1% or 1:1000 women. There were 31 pregnancies amongst these 14 women, and therefore the prevalence of seropositive pregnancies was 0.03% (3:10 000 pregnancies). The remainder 15 women (51.7%) were false positives to HIV on initial screening.
Eleven (78.6%) out of the 14 patients were known HIV carriers and three (21.4%) of the 14 women were newly diagnosed cases at the time of first presentation (not known before having HIV), as shown in Figure 1.
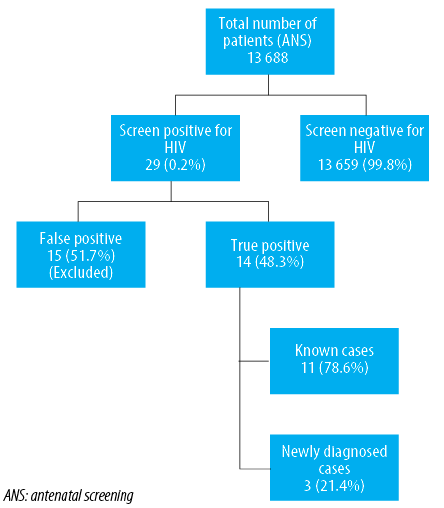
Figure 1: Demonstrates the total number of true HIV-positive women during the study period and further divides them into known and unknown cases.
Of the 31 pregnancies, there were three (9.7%) miscarriages and 28 (90.3%) live births. All of the miscarriages were known to have HIV, with singleton pregnancies, and presented in their first trimester. All (100%) were on ART from the first trimester and miscarried during the first trimester. One of three was medically managed with misoprostol, one was surgically managed with suction evacuation, and no data was available for the third miscarriage. The viral load was < 1000 copies/mL and in fact undetectable (< 50 copies/mL) and the CD4 count was > 500 cells/mm3 in two-thirds of cases. No data was available for the third miscarriage.
Of the 28 live births, three (10.7%) had unknown HIV status as they presented in the third trimester during active labor. Routine ANS identified them as seropositive. All were singleton pregnancies and did not receive antenatal ART due to their unknown status. One in three (33.3%) had a normal vaginal delivery, while the remaining two (66.7%) resulted in emergency cesarean section (one with suspected chorioamnionitis and the other in breech position). There were no known antepartum complications, confounding factors, or known acquired infections. One of the three had intrapartum fever (suspected chorioamnionitis). None of the patients received intrapartum ART prophylaxis due to their unknown status, while 66.7% suffered from puerperal fever (one who delivered by emergency cesarean section for suspected chorioamnionitis, while the other normal vaginal delivery suffered from breast engorgement).
The mean gestational age at delivery was 39.6±0.5 weeks gestation (range = 39–40 weeks) with a mean birth weight of 3.2±0.35 kg (min 2.9 kg, max 3.6 kg). All three were advised to breastfeed as per routine, and all were advised to discontinue breastfeeding and offered cabergoline after ANS revealed positive status for HIV. One patient refused to stop breastfeeding.
All three neonates were born females with Apgar scores of 9 and 10 at one and five minutes, respectively, and none required admission to the NICU post-delivery. Two out of three babies (66.7%) received postnatal ART, with one (33.3%) testing positive for HIV. None had visits to the emergency room, and only 33.3% had an outpatient department visit to follow-up on HIV status (one did not attend their appointment, whereas the other was lost to follow-up).
The viral load of the mother with a seropositive infant after birth was 4644 copies/mL with a CD4 count of 395 cells/mm3. The viral load of the other mother who had a spontaneous vaginal birth was 22 333 copies/mL with a CD4 count of 401 cells/mm3. The third unknown HIV patient (who delivered by emergency cesarean for breech labor) had no documented viral load/CD4 count post-delivery.
Of the 25 known HIV-positive pregnancies, 16.0% presented in the first trimester, 68.0% in the second trimester, and 16.0% in the third trimester. All known cases were followed up with the infectious disease team. All were on ART during pregnancy. Eighty percent were on ART before pregnancy,
4.0% were started in the first trimester, and 16.0% started in the second trimester. With regards to compliance to medication, 87.0% were compliant with their medication.
Table 1 illustrates the percentage of patients according to viral load and CD4 count per trimester.
Of the 25 pregnancies, 96.0% were singleton with one set of twins (4.0%). With regards to the mode of delivery, 45.8% had spontaneous vaginal delivery, 8.3% were induced (one for postdate and the other for unprovoked deceleration), 20.8% had elective cesarean section (for previous cesarean section, fetus with intrauterine growth restriction (IUGR), and diaphragmatic hernia), and 25.0% had emergency cesarean sections (one for previous two cesarean sections in labor-twin pregnancy at 33 weeks gestation, was booked for elective cesarean but attended with preterm labor, one was breech in labor (also booked for elective cesarean section), two with premature rupture of membrane and prolonged latent phase, and one with preterm labor with uncontrolled retroviral disease).
Table 1: Percentage (%) of patients according to viral load and CD4 count per trimester.
|
First |
61.9 |
38.1 |
46.7 |
53.3 |
|
Second |
100 |
0.0 |
41.2 |
58.8 |
*A viral load of < 1000 is considered suppressed.
** A CD4 count < 500 is considered immunocompromised.
The vast majority (72.0%) had no obstetrical cofounding factors, 8.0% had diabetes mellitus, 4.0% with gestational diabetes, 4.0% with obstetric cholestasis, and 12.0% had other factors such as iron deficiency anemia, chronic idiopathic thrombocytopenic purpura, and fundal fibroid uterus.
With regards to antepartum complications, 40.0% had no antepartum complications, 20.0% had vaginal infections (e.g., candidiasis), and 40.0% had other complications which included; 40.0% IUGR/small for gestational age (SGA), of which 25.0% had associated diaphragmatic hernia, 10.0% with carpal tunnel syndrome, 10.0% admitted for glycemic control associated with hypokalemia, 10.0% with fetal pelvi-ureteric junction dilatation, 20.0% with threatened preterm labor of which 50.0% were associated with thrombocytopenia and pyelonephritis.
Regarding acquired opportunistic infections (Pneumocystis jirovecii pneumonia, Mycobacterium avium complex), 4.0% suffered from pneumonia, but this was deemed community acquired. The majority (75.0%) did not suffer from intrapartum complications, 4.2% suffered from intrapartum pyrexia (patient with pyelonephritis), and 20.8% from others such as meconium-stained liquor (83.3%) and preterm premature rupture of the membrane (PPROM) at 37 weeks gestation (16.7%).
All patients received intrapartum ART prophylaxis. Two-thirds (66.7%) had no postpartum complications, while 4.2% had postpartum hemorrhage, 4.2% had puerperal fever, 8.3% had anemia, and 16.7% had other complications such as first degree perineal tear (25.0%), second degree perineal tear (25.0%), urinary tract infection post cesarean section (25.0%), and 25.0% with pulmonary edema and hypertension (suspected congestive cardiac failure).
Only 92.0% were advised to refrain from breastfeeding, with an alarming 8.0% advised to breastfeed, which was documented in the patient’s notes. Nonetheless, they were subsequently asked to refrain from breastfeeding once HIV status was alerted.
The mean gestational age at delivery was 37.4±1.9 weeks (range = 33–40 weeks gestation), 36.0% of which were preterm deliveries (< 37 completed weeks of gestation).
There was a total of 26 neonates (one set of twins), two of which were delivered elsewhere, so the following results are of the remaining 24 neonates.
The mean birth weight was 2.6±0.5 kg (range = 1.5–3.8 kg). Half of the neonates were male and half female. All had an Apgar score ≥ 6 at one minute and ≥ 8 at five minutes.
All neonates received postnatal ART prophylaxis and tested negative for HIV post-delivery. One-third of the neonates (33.3%) required NICU admissions, and four neonates (18.2%) attended the emergency room. The majority (81.8%) attended outpatient department follow-up further repeat testing of HIV status.
Discussion
The prevalence of HIV in pregnant women during the study period was comparable to the preceding 10 year study at SQUH from 1995 to 2005 (prevalence of 0.1% and 0.13%, respectively). This value was 10-times higher than the national prevalence of HIV in pregnant women conducted by the Oman MOH (0.02%) during the screening period between 2009–2014, but still in keeping with the national prevalence of the general population of < 1.0%.10
Surprisingly, there was a high false-positive rate on initial testing (51.7%), which was identified after 2011. After further investigations, it was noted that there was an upgrade to fourth generation enzyme-linked immunosorbent assay by the hospital laboratory, which deemed it more sensitive but not more specific to HIV than previous tests.
These false-positive results were included in our initial assessment of prevalence, as we aimed to identify those who had a positive result in the ANS, but were excluded in our analysis, as they would subsequently obscure the true results and analysis of MTCT.
The prevalence of miscarriages amongst the total number of HIV positive pregnancies was 9.7%, which reflects the general background miscarriage rate of 10%–20%11 and is unlikely to be related to HIV as these patients were appropriately managed before and during their antenatal period, and compliant to medications which was reflected on their suppressed viral loads at the time of miscarriage.
When looking at the unknown HIV-positive women who did not receive any prenatal care at SQUH, all delivered to term with appropriate birth weights for gestational age and Apgar scores. The indications for cesarean sections were warranted for obstetrical and fetal causes. It comes as no surprise that the neonate born with HIV was from the patient who had an emergency cesarean section for suspected chorioamnionitis. Despite receiving postnatal ART, the patient refused to refrain from breastfeeding and refused cabergoline use, which further added to the MTCT. Nevertheless, with no intervention, the MTCT was 33.3%, which reflects the background transfer of HIV by MTCT in the absence of intervention.4
Only one-third of these infants born to HIV-positive patients were followed up in the SQUH outpatient department. Ideally, all infants born to seropositive women are routinely followed up to 18 months regardless of their status. The infant that was followed up was the one who tested positive initially and was further referred to a pediatric tertiary center for communicable diseases. The poor follow-up for the other two infants was a result of missed appointments by parents who left against medical advice post-delivery, and one loss to follow-up who was detected again at two years of age by the family screening program.
Regarding the known HIV-positive women, 84.6% were seen in the outpatient department by the end of the second trimester. This is seen as ideal as a referral from the infectious disease department to OBGYN aims for the patient to be referred once pregnancy is identified and to be seen once viability is confirmed for management of pregnancy and labor and breastfeeding advice. With regards to the remainder 15.4% seen in the third trimester, one missed her second trimester appointment and attended in active labor, two had no follow-up and attended during their third trimester in active labor, and one received a late appointment at 34 weeks.
The compliance rate to ART in this cohort was 87.0%. The reasons noted for non-compliance to medications were change in medications, side effects such as diarrhea and vomiting, dizziness, abdominal pain, and low socioeconomic class.
When looking at the viral load in each trimester, 92% were suppressed to undetectable levels by the third trimester.12
With regards to the mode of delivery, the vast majority had vaginal births. Cesarean sections were related to obstetrical and fetal factors rather than HIV per se. The exception was for the emergency cesarean section done for a patient with uncontrollable retroviral disease. This patient was non-compliant with her medications due to personal reasons and vomiting. She had a viral load of 63 681 copies/mL and a CD4 count of 123 cells/mm3 in the third trimester. As a strategy to prevent MTCT, cesarean section was done to minimize the risk of transfer.
Similarly, most patients had no confounding factors, whereas 12.0% exhibited anemia of pregnancy, which, as mentioned previously, may have an increased risk of development due to HIV status. This was demonstrated in the study done in a tertiary hospital in Nigeria published in 2015 where a significant percentage (8.1%) of seropositive pregnant women had anemia compared to the control group (3.1%).8 However, it is not unusual to have anemia in pregnancy. According to the WHO criteria, 52% of pregnant women from undeveloped or developing countries are anemic compared with 20% from industrialized nations. This is mainly attributed to high fetal demands for iron and render iron deficiency, the most common cause of anemia in pregnancy, with other causes contributing less frequently.13
Similarly, a common antepartum complication of pregnancy, experienced by a fifth of the patients, are vaginal infections, particularly candidiasis. It is recognized that approximately 20% of asymptomatic women have vaginal colonization with candida, and there is a 30%–40% increased rate of colonization in pregnancy and uncontrolled diabetes. In addition to immunosuppression and antimicrobial therapy, these factors attribute to symptomatic candidiasis.14 Therefore, we cannot conclude that HIV status alone is the direct cause of vaginal infections in the 20.0% of pregnant women in our study. The same is true for the SGA/IUGR fetuses where congenital infections such as Toxoplasma gondii, rubella, cytomegalovirus, herpes simplex virus, varicella-zoster virus, Treponema, and HIV only contribute to 5%–10% of fetal growth restriction, whereas maternal diseases such as anemia of pregnancy and malnutrition and uteroplacental dysfunction in which pre-eclampsia and abruption come under have a wider role.15
Fortunately, there were no documented opportunistic infections in the seropositive pregnant women, which reflect the good compliance to medication, with suppressed viral loads and immunocompetence.
When looking at the intrapartum complications, only 4.2% suffered from intrapartum pyrexia - the source of infection identified from the data as pyelonephritis. One-fifth with meconium-stained liquor and 16.7% with PPROM. Again, multiple factors could lead to this, the normal process of labor and stresses of labor being some.
SQUH has shown excellent management of these seropositive women during active labor, where all received intrapartum ART prophylaxis and postnatal ART prophylaxis. It was unfortunate that 8.0% of the patients were advised as routine to breastfeed. Still, if we look at the Swiss cheese model of accident causation, they were eventually picked up in time to advise to stop, and this would be considered a near miss, as none of the neonates were affected by HIV.
The postpartum complications that occurred are no different from the general population. One thing to note is postpartum hemorrhage. SQUH practices delayed cord clamping during active management of the third stage of labor. Concerns regarding this could be raised given the belief that delay in the separation of the placenta may increase the exposure of the fetus to maternal blood. The WHO recommendation for prevention and treatment of postpartum hemorrhage has stated that the proven benefits of a 1–3 minute delay in clamping the cord outweigh the theoretical, and unproven harms, and late cord clamping is recommended even among women living with HIV or women with unknown HIV status as long as there is no acute feto-maternal compromise.16
With regard to preterm delivery, 36.0% were delivered at < 37 weeks gestation. This included the twin pregnancy presenting at 33 weeks with labor pains, an emergency cesarean was done for her given her obstetrical history of three previous cesareans. This, in turn, skewed the mean gestational age at delivery and mean birth weight in view of preterm and twins (1.5 kg and 1.7 kg, respectively). Likewise, two other 33 weeks gestation fetuses resulted in emergency cesarean section; one for breech in labor (birth weight 2.1 kg) and the other for preterm labor with uncontrolled retroviral disease mentioned previously (birth weight 2.0 kg). Therefore, when looking at the mean gestational age, as well as birth weight, we are more inclined to attribute it to obstetrical factors rather than HIV, with the exception of the last patient. To justify this, although preterm births are higher in HIV positive cohort as shown in the Nigerian study compared to the control group, ART reduced the risk of preterm birth in the HIV positive cohort,8 which our patients were all taking.
The NICU admissions were for small gestational age neonates, prematurity, presumed sepsis, respiratory distress, and congenital diaphragmatic hernia (CDH) with multiple birth defects. The emergency attendance was due to suspected sepsis (norovirus at five weeks age, and another with CDH/multiple congenital disabilities), one at eight months with viral upper respiratory tract infection, and one with community-acquired pneumonia.
With regard to outpatient department follow for HIV status monitoring, the following infants had regular follow-up for pelviureteric junction dilatation and hydronephrosis; persistent metabolic acidaemia to a mother with systemic lupus erythematosus/Sjögren syndrome; megameatus for circumcision at nine months; stridor with no cardiac cause; left congenital diaphragmatic hernia with pulmonary hyperplasia, multiple jejunal perforation, cholestasis, delayed milestones, and dysmorphism.
Looking at birth defects, we cannot conclude HIV as direct cause per se in this study. However, the fetus with multiple congenital anomalies — born with left CDH, pulmonary hyperplasia, multiple jejunal perforation, cholestasis, delayed milestones, and subtle dysmorphism — was born to a mother who was on Trizivir (a combination of abacavir, lamivudine, and zidovudine) before pregnancy. Looking at the Food and Drug Administration label; data available from the Antiretroviral Pregnancy Registry show no difference in the overall risk of birth defects for Abacavir, Lamivudine, or Zidovudine compared with the background rate of 2.7%.17 Therefore, these birth defects are unlikely related to the medication administered.
Conclusion
Strategies have been placed by programs in Oman to focus on pregnant women’s wellbeing and the protection of newborns against HIV infection. By strict implementations on preventing MTCT, preventing HIV in children has become possible. ART significantly reduces vertical transmission of HIV, in addition to abstinence of breastfeeding. An established interaction between researchers, clinicians, healthcare workers, and pharmacists has provided better care for mothers and their children. More importantly, all HIV-positive pregnant women should follow the prevention of MTCT programs set out by the MOH, and their male partners should be involved in antenatal care.
This study focused on pregnant women presenting at a single center which is a tertiary care facility, rather than a multi-center trial. The disease under investigation is of low prevalence nationally, and therefore, analysis of results was limited to the low number of cases obtained. Not all deliveries were conducted in the center, and there was a high level of loss to follow-up due to individual and structural factors.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
references
- 1. Shaw GM, Hunter E. HIV transmission. Cold Spring Harb Perspect Med 2012 Nov;2(11):a006965.
- 2. World Health Organization. HIV/AIDS. [cited 2018 Aug 17]. Available from: http://www.who.int/news-room/fact-sheets/detail/hiv-aids.
- 3. amfAR: statistics: women and HIV/AIDS: the foundation for AIDS research: HIV / AIDS research. [cited 2018 Aug 17]. Available from: http://www.amfar.org/about-hiv-and-aids/facts-and-stats/statistics--women-and-hiv-aids/.
- 4. Cohn SE, Clark RA. Human immunodeficiency virus infection in women. In: Mandell, Douglas, and Bennett’s principles and practice of infectious diseases, updated edition. 8th ed. Philadelphia, PA: Elsevier/Saunders; 2015. p. 1590-1615.e10.
- 5. Department of Health Information and Statistics. Directorate General of Planning and Studies. Annual health report 2019. Sultanate of Oman: Ministry of Health; 2019.
- 6. Jaffer YA, Al-Awaidy ST. Elimination of mother-to-child transmission of HIV, an experience from Oman. J HIV AIDS 2017 Jan;3(1).
- 7. Al-Jabri AA, Al-Muharrami ZK, Balkhair AA, Ganguly SS. The importance of HIV antenatal screening programs for pregnant women. Saudi Med J 2010 Jan;31(1):64-68.
- 8. Ikpim EM, Edet UA, Bassey AU, Asuquo OA, Inyang EE. HIV infection in pregnancy: maternal and perinatal outcomes in a tertiary care hospital in Calabar, Nigeria. Trop Doct 2016 Apr;46(2):78-86.
- 9. Li N, Sando MM, Spiegelman D, Hertzmark E, Liu E, Sando D, et al. Antiretroviral therapy in relation to birth outcomes among HIV-infected women: a cohort study. J Infect Dis 2016 Apr;213(7):1057-1064.
- 10. Al Awaidy ST, Sharanya A. Successes and challenges of HIV/AIDS program in Oman: 1984-2015. Oman Med J 2019 Jan;34(1):1-8.
- 11. Keyhan S, Muasher L, Muasher SJ. Spontaneous abortion and recurrent pregnancy loss: etiology, diagnosis, treatment. In: Comprehensive gynecology. 7th ed. Philadelphia, PA: Elsevier; 2017.
- 12. Gray GE, McIntyre JA. HIV and pregnancy. BMJ 2007 May;334(7600):950-953.
- 13. Lee AI, Okam MM. Anemia in pregnancy. Hematol Oncol Clin North Am 2011 Apr;25(2):241-259.
- 14. Magowan B, Owen P, Thomson A. Pelvic infection and STIs. In: Clinical obstetrics and gynaecology. 4th ed. Elsevier; 2019. p. 155-168.
- 15. Schlaudecker EP, Munoz FM, Bardají A, Boghossian NS, Khalil A, Mousa H, et al; Brighton Collaboration Small for Gestational Age Working Group. Small for gestational age: case definition & guidelines for data collection, analysis, and presentation of maternal immunisation safety data. Vaccine 2017 Dec;35(48 Pt A):6518-6528.
- 16. World Health Organization. WHO recommendations for the prevention and treatment of postpartum haemorrhage. 2012 [cited 2019 November 21]. Available from: https://www.who.int/reproductivehealth/publications/maternal_perinatal_health/9789241548502/en/.
- 17. Trizivir FD. Label - Tablet (film coated). AIDSinfo. [cited 2019 Nov 20]. Available from: https://clinicalinfo.hiv.gov/en/drugs/abacavir-lamivudine-zidovudine/patient.