|
Abstract
Objective: This study aims to measure the rate, types, and causes of injuries presented at a primary care setting in the Muscat governorate.
Methods: A cross-sectional study was carried out where all patients who attended the Al Moabelah Health Center from the period of 1st January 2010 to the 31st December 2010 were identified from the electronic medical records. Patients identified with any type of injury were then selected for further data collection with their age and gender recorded. Details such as the type, cause and nature of the injury at the clinic were gathered from the clinical notes.
Results: A total number of 86,554 visits were recorded for the year 2010. The rate of injury visits was 24 per 1000 visits. In this study, the rate of injury visits was found to be four times more common in males (44.4 per 1000) than in females (11.5 per 1000), p≤0.001.While children aged under 12 years accounted for 41.4%, and elderly patients aged over 60 years accounted for 3.5% of the total visits emanating from injuries. The results show that home was the most common place where the majority of injuries occurred (42%), followed by playgrounds (10.2%). The most common causes of injury visits were falls, followed by cutting/piercing by sharp objects and sports injuries, which accounted for 40%, 13.4%, and 12%,respectively.
Conclusion: Injuries in a primary care setting with close proximity to emergency departments of secondary and tertiary hospitals may only account to less than 3% of the total visits.
Keywords: Injuries; Primary care; Oman; falls.
Introduction
Injuries are among the most common preventable health problems worldwide. According to the World Health Organization (WHO), injuries account for 9% of global mortality annually with more than five million cases reported resulting from different kinds of injuries.1 Furthermore, 15% of global Disability-Adjusted Life Years (DALY) losses were directly linked to injuries.2 By the year 2020, the proportion of DALY related to injuries is expected to increase considerably and is estimated to contribute to 20% of all DALY losses.2 Indeed, injuries are still considered to be a major cause for consultation at primary care settings and emergency departments leading to hospitalizations.3
In the Sultanate of Oman, road traffic injuries (RTI) in particular, contribute substantially to the high rates of morbidity and mortality.4 In the year 2008, DALYs resulting from injuries in Oman were estimated to be approximately 5.7 DALY per 1000 capita.5 In 2009, the outpatient morbidity from injuries accounted for 4.4% of the total number of patients presented to primary care institutions and 7.6% of the total hospital admissions.6 Easy access to healthcare services for patients and their families is the hallmark of the primary care system.7 For this reason, primary care centers have become the first point of contact for the majority of emergency cases, including injuries.8 In Oman, the accessibility of primary healthcare to the general population has ensured the integral role exhibited by primary care centers in the management of some emergency cases such as injuries.6
Although for many years now, Oman has had a well-established primary healthcare system, the epidemiologic profile of all related injuries in primary care settings has not been explored. This paper intends to determine the visits rate, type, and cause of injuries presented to a primary care center in the Muscat governorate.
Methods
This cross-sectional pilot study was conducted between 1st January 2010 and 31st December 2010 at a health center (Al Moabelah) in the Muscat governorate. This health center is one of the largest in the country and serves a heterogeneous population in terms of socio-demographic characteristics of more than 40,000 persons. As with other health centers in Oman, this health center operates from 7:00 am to 9:00 pm from Saturday to Wednesday, and between 9:00 am and 4:00 pm during the weekend. It is located within 20 km of major hospitals in Muscat, Sultan Qaboos Univeristy Hospital, and Arm Force Hospital.
For the purpose of the study, injury was defined as “damage or harm done to or suffered by a person causing the person to seek medical care.” Data were retrieved from the Electronic Medical Records System (Al-Shifaa) for all patients who had attended the health center and presented with injuries (as previously defined) during the study period. In retrieving the relevant patient data, all related codes under the classification of injuries were used to search for the diagnosis (ICD-10) of the injuries, including fall, trauma, burns, road traffic accidents, fractures, wounds, sprains, strains, dislocations, concussions, and acute poisonings (except those caused by contaminated food) resulting from exposure to toxic or poisonous substances. The rate of circumstances and causes, as well as the nature, treatment and disposition of injuries treated at the health center were extracted from the clinical notes. All injury visits were collected and patients who had more than one visit for the same injury was considered as one visit only. The data was collected by two medical doctors who were trained to use the Al-shifa system. Data was entered and analysed into SPSS version 19. For the purpose of analysis, the yearly rate of all injury visits was calculated per 1000 visits. The study was ethically approved by the Ministry of Health (MOH) research and ethics committee.
Results
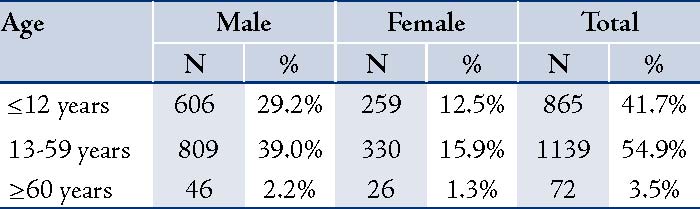
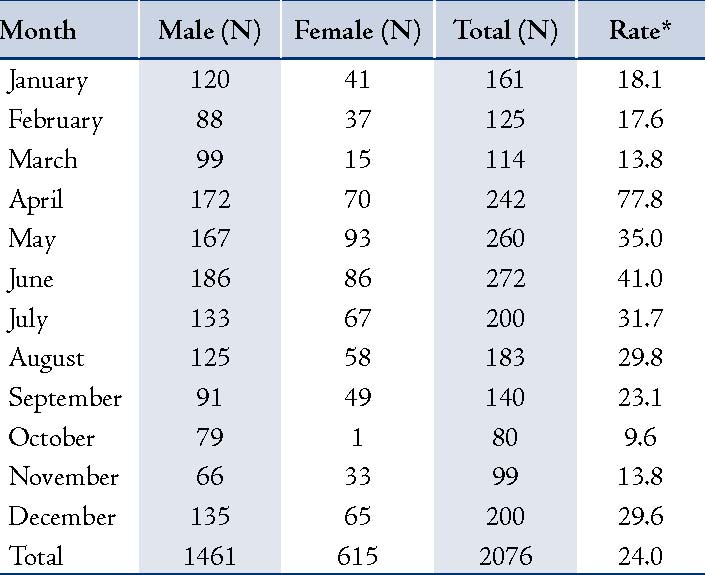
The total number of visits to the health center by all patients in year 2010 was 86,554, while the total number of visits related to injuries was 2076 (24 per 1000 injury visits). The age of the studied population ranged between 2 months and 96 years, with an average age of 20.3 (SD=17.5) years. The study population was composed of more males (n=1461; 70.3%) than females (n=615; 29.7%), thus the rate of injury visits was four times higher in males (44.4 per 1000 visits) than in females (11.5 per 1000 visits), p≤0.001. The majority of injuries affected children. The 13-59 age group accounted for 54.9% of the total visits linked to injuries, while elderly patients aged ≥60 years constituted only 3.5% of the total visits linked to injuries, (Table 1). The highest rates of visits related to injuries were observed during the months of April, May, and June (77.8, 35.0, and 41.0 per 1000 visits, respectively) while the lowest rates were recorded during the months of October and November (9.6 and 13.8 per 1000 visits, respectively). (Table 2)
Table 1: Frequency and percentage of injury visits according to age groups.
During the months of January and April, a considerable proportion of the injuries occurred at school (22.8% and 15.8%, respectively), while the majority of injuries were reported to have occurred at home between the months of June and July (16.2% and 11.2%, respectively), p≤0.001. On the other hand, most of the injuries reported during the months of April (15.9%) and May (15.1%) were linked to sports and most injuries reported to have occurred during the months of May (10.9%) and June (11.0%) were attributed to falls, (p≤0.001). The study revealed that the most common places where the majority of injuries were reported to have occurred were home (42.3%), street/playground (10.4%), and at school/ work 3.0%. Moreover, the highest rate of injuries reported to have occurred at home were accounted for males (24.6%) compared to females (10.7%; p≤0.001); however, elderly patients were most notably associated with injuries reported to have occurred at home (63.5%), overall.
Table 2: Frequency and rate of injury visits according to the month of occurrence.*(rate of injury visit/1000).
According to the results, the most common causes of injury visits were falls (40.3%); followed by cutting/piercing by a sharp instrument (13.4%); sports (12.7%); struck by or struck against objects (12.4%); fire/chemicals (5.7%), RTAs (3.6%); assault and abuse (2.4%); drug/substance overdose (1.2%); and bites/stings (0.2%). However, there were no documentations alluding to the causes of injury visits in 8.4% of cases. Based on the study results, males (26.0%) constituted a significantly higher rate of falls than females (14.2%; p≤0.001), and 19.9% of injuries linked to falls were reported in patients aged ≤12 years, (Table 3). Generally, the injury visits in male patients mostly resulted in superficial wounds (28.6%) and strains/sprains (20.9%); whereas in females, the injury visits mainly resulted in contusions/ hematomas (22.3%) and sprains/strains (20.8%; p≤0.001). Moreover, burns were more frequently reported in females compared to males (9.6% and 3.3%, respectively; p≤0.001). (Table 4)
In terms of the site of injury; the lower extremities of the body were mostly affected (39.6%), followed by the upper extremities (30.8%). The face was affected in 11.5% of cases, followed by the scalp and neck (9.5%); however, facial injuries were most commonly seen in the pediatric age group (20.5%). Of the total number of patients who visited the clinic as a result of injuries, 37% had X-ray of bones upon initial evaluation, of which only 2.9 % showed fractures in the extremities. Overall, the majority of cases (90.8%) were discharged home without need for follow-up visits; hence, only 9.2% of all the reported injuries (which were mostly cases of fracture) were referred to tertiary care hospitals.
Table 3: Place of injury according to age groups and gender.
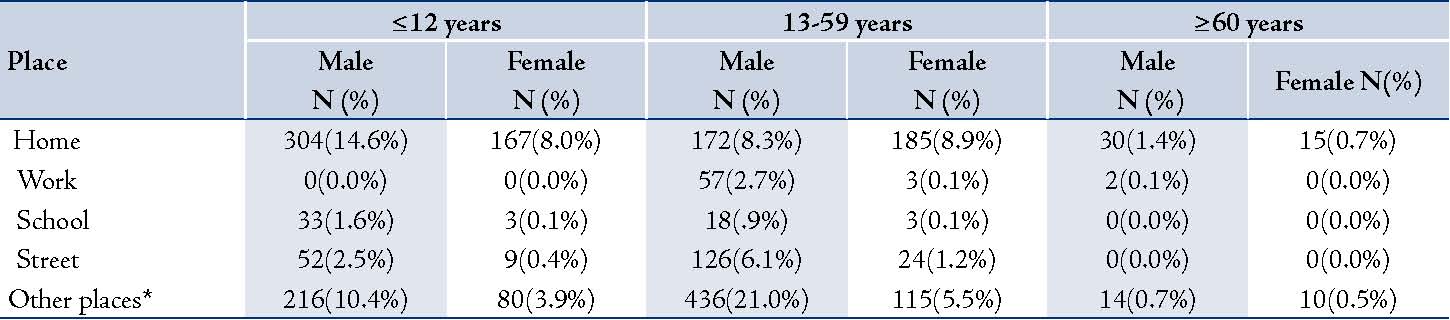
*Other places: playgrounds, farms, beachs, sea.
Table 4: Cause of injury visits according to age group and gender.
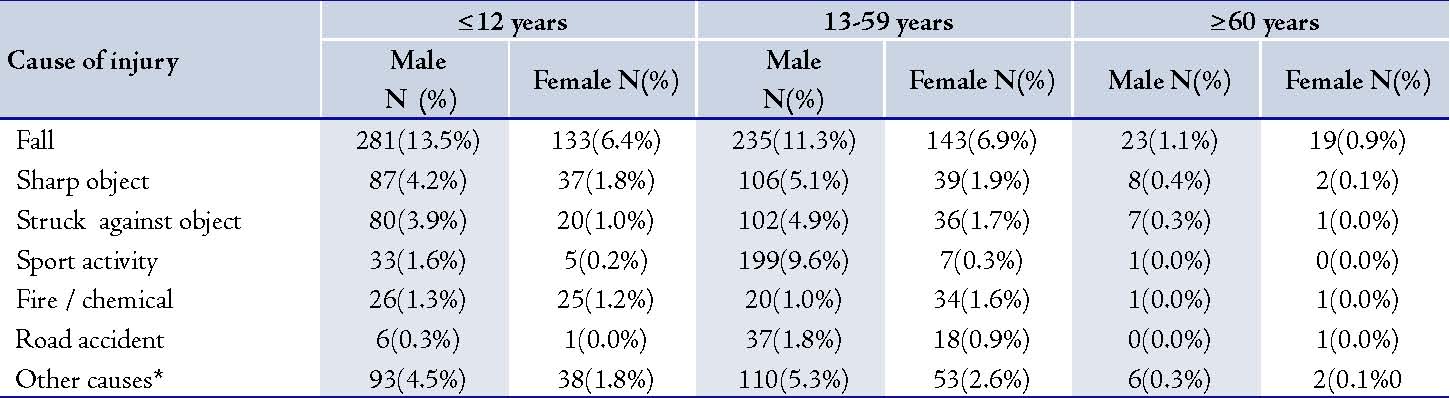
* Other causes include: stings, bites, assault, drug/substance abuse, & undocumented.
Table 5: Nature of injuries according to age groups and gender.
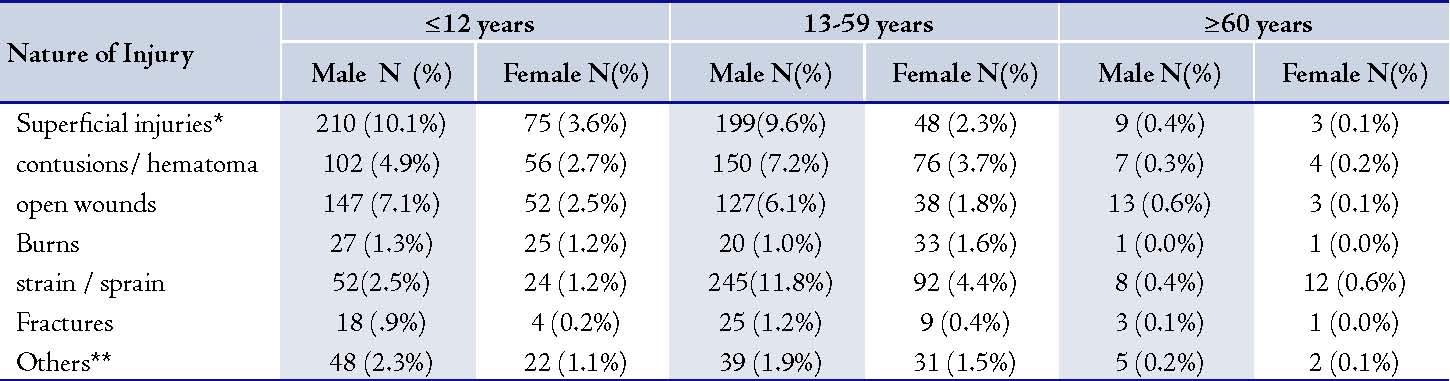
* including lacerations & abrasions.
** including: drug/substance overdose, abuse, & undocumented data about the nature of injury
Discussion
Research on injuries in primary care settings is generally scarce; hence this pilot study was aimed at examining some of the features related to injuries presenting to a primary care center in Oman. The health center selected for this study has one of the highest population coverage in the Muscat governorate. The rate of injury visits presented at this center was 24 per 1000, which is far less than the reported rate of injuries in the overall healthcare institutions according to the ministry of health (640/1000).6 The difference in rate can be attributed to the fact that injuries are mostly escorted and managed in secondary and tertiary care hospitals in Oman, which are open 24 hours, seven days a week.6 In addition, most of the injuries presented at the health center in this study were minor injuries such as falls, sports related activities and lacerations, as well as hematomas and strains. Serious injuries such as road traffic injuries tend to be immediately transported to the emergency departments of the major hospitals. In fact, the incidence of RTAs reported in the current study (3%) is considerably lower compared to the value reported in the 2009 National Health Report (21%) for the total external causes of outpatient morbidities at Ministry of Health (MOH) institutions.6 This may also be attributed to the use of private sector establishments in the same area.
In this study, a higher number of injury visits was observed among adult males compared to adult females; this finding is consistent to other studies reported elsewhere.9,10 The possible explanation for this could be the fact that males most commonly tend to be outdoors compared to females; and the risks of injury outdoors are much greater. In our study for instance, adult females were most commonly implicated in injuries reported to have occurred at home such as burns, wounds from cuts and falls, while males were mainly associated with sports-related injuries. This may possibly be attributed to the gender-specific roles in the cultural context of Oman, where males hold more responsibilities for socially related outdoor activities compared to females.11,12 13 In this study, the difference in the pattern of injury visits between adult males and adult females was also conveyed in the pediatric age group, which coincides with national and international findings.6,11,12,14 Children are usually at higher risk of being exposed to injuries because of their increased physical activity, mental immaturity and risk-taking behaviors.15,16,17
Although childhood injuries should be prevented whenever possible due to higher mortality and morbidity,18 still the rate reported in the current study was high (41% of total visits due to injury). Studies in the USA have also reported the childhood (0-14 years) injury rate to be 139/1000s (13.9%),9 while in the UK, the annual rate of injuries amongst children (0-15 years) who attended either General Practice or Emergency Departments was one in five (20%).20 However, this comparison may not be fair as the age categories used are not the same across the countries, as well as the international figures included injuries presented at all levels of care. Therefore, a study is needed to explore potential risks at homes in Oman that could result in childhood injuries. Moreover, primary healthcare professionals could start some health promotional activities to parents, especially mothers visiting healthcare centres on how to avoid childhood injuries and minimize causes of risk of injuries at home.
The most common causes of injury visits were falls followed by cutting/piercing by a sharp instrument. Globally, falls are a major public health problem and fatal falls is the second leading cause of unintentional injury deaths after road traffic injuries and responsible for 17 million disability-adjusted life years (DALYs) lost.21 For the year 2010, according to the National Estimates of the 10 Leading Causes of Nonfatal Injuries Treated in Hospital Emergency Departments in the United States, unintentional falls ranked first for all age groups; cutting/piercing was the third among 5-9 years age group after unintentional struck.22 There are several reasons attributed to the increased incidence and prevalence of unintentional falls compared to other types of injuries across all age groups. Older people are at an increased risk of falls (with subsequent hip fractures or head traumas) mainly due to physical, sensory, and cognitive changes associated with ageing. On the other hand, childhood falls (with subsequent face and scalp traumas) occurred largely as a result of their evolving developmental stages, innate curiosity of their surroundings, increasing levels of independence and inadequate adult supervision.21
This study was not without limitations, however, and the major limitation could be regarded as the tendency to generalize and extend the study findings to other primary care centers in the country. Since this was only a study conducted at one health center, the findings are therefore limited to that one center and cannot be generalized to other settings. In addition, the health center is located in the Muscat governorate, where emergency services of secondary and tertiary hospitals are in close proximity. Therefore, the current figures may not be consistent with figures from other health centers, which are not within close range to emergency departments of secondary and tertiary care centers. The data obtained in this study was based on retrospective record review. Many other important variables cannot be obtained as clinical notes were not complete. Another limitation of this study was that it examined injury visits not injuries per say. Few patients would sustain a higher risk of having more than one injury during the same year. Furthermore, some injuries, particularly occupational injuries might be managed at private settings. The category of <12 years comprises a wide range of age groups and there could be no differences in behaviors between genders in the earlier years of childhood. Thus, the category could not be further subdivided due to limitations of the Al-Shifa system.
Therefore, commencing a national injury survey which will encompass a representative sample of both public and private healthcare settings in the country, in addition to a household injury survey in order to construct a clearer insight into common injuries, their potential causes and consequences, in the country is recommened.
Conclusion
Injuries in a primary care setting with a close proximity to emergency departments of secondary and tertiary hospitals may only account to less than 3% of the total visits. The study found that adult males and children are at a higher risk of encountering injuries compared to adult females and elderly patients; however, further research is needed to investigate the burden, causes and consequences of injuries presenting to primary care facilities in Oman.
Acknowledgements
The authors reported no conflict of interest and no funding was received in this work.
References
1. Scott D, Donald J, Vincent A. Disability and Disability-Adjusted Life Years: Not the Same. Public Health Rep 2000;124:197-202.
2. Taker A. Accident mortality in children, adolescent and young adults. World health stat Q1986;39:232-56.
3. Gallagher SS, Finison K Guyer BF, Goodenough S. The incidence of injury among 87000 Massachusetts children and adolescents: result of 1980-81 statewide childhood injury prevention program surveillance system. Am public Health 1984;74:340-7.
4. Al-Azri NH. . Emergency medicine in Oman. . Int J Emerg Med 2009 11 Dec 2009;2(4):199-203.
5. Ministry of Health, sultanate of Oman. Health Status Indicators. 2009; Available at: http://www.moh.gov.om/en/stat/2009/index_eng.htm. Accessed Sept/10, 2010.
6. Jawad A Al-Lawati, Ruth Mabry, Ali Jaffar. Addressing the Threat of Chronic Disease in Oman. 2008; 5:A99. Prev Chronic Dis 2008;5(99).
7. Ashwani Dhar. Medical Informatics and Health Care in Oman. 2001: 8 : 515-517 J Am Med Inform Assoc 2001;8(515-517).
8. WHO. Alma Ata: Primary Health Care". HFA Sr 1978;1
9. Arntson P. Improving Citizens’ Health Competencies. 1989;1:29-34. Health Communication 1989;1:29-34.
10. WHO. Child and adolescent injury prevention: A Global Call to action. Available at: http://whqlibdoc.who.int\publications\2005\9241593415_eng.pdf. Accessed June/5, 2010.
11. Baker SP, Harvey AH. Fall injuries in elderly. Geriatric Medicine 1985;1:501-512.
12. Alexander C, Somerfield M and Ensminger M. Gender differences in injuries among rural youth. InjPrev 1995;1:15-20.
13. Bem SL. Gender schema theory: A cognitive account of sex typing. Psychological Review 1981;88:354-364.
14. Hartzog T, Timerding B, Alson B. Pediatric trauma: enabling factors, social situations, and outcome. AcadEmerg Med 1996;3:213-220
15. Farrington DP LR.Epidemiology of juvenile violence. Child adolesc psychiatr clic N Am 2000;9:733-748.
16. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. 1986; Available at: http://hsc.usf.edu/~kmbrown/Social_Cognitive_Theory_Overview.htm. Accessed Dec/10, 2010.
17. Woods M. Injury a leading killer for children in Asia. 2008; Available at: http://www.abc.net.au/rn/breakfast/stories/2008/2192680.htm. Accessed October/6, 2010.
18. Morrongiello A, Lisa Ondejko MA, Littlejohn A. Understanding toddlers In-Home I njuries. 2004:29 ; 433-446. J Pediatr Psychol 2004;29:433-446.
19. Center for disease control and prevention, national center for injury prevention and control. Web-Based injury statstics query and reporting system (WISQARS) 2007; Available at:http://www.cdc.gov.myaccess.library.utoronto.ca/injury/overview. Accessed march/20, 2010.
20. Agass M, Mant D, Fuller A, Coulter A, Jones L. Childhood Accidents: a practice survey using general practitioners' records and parental reports. Br J Gen Pract 1990;40:202.
21. World Health Organization (WHO). Media Center, Falls Fact Sheet No 344, August 2010, WHO. http://www.who.int/mediacentre/factsheets/fs344/en/index.html. (Accessed 21.9.2012)
22. Office of Statistics and Programming, National Center for Injury Prevention and Control. National Estimates of the 10 Leading Causes of Nonfatal Injuries Treated in Hospital Emergency Departments, United States – 2010. The Centers for Disease Control and Prevention (CDC), USA http://www.cdc.gov/Injury/wisqars/pdf/National_Estim_10_Leading_Causes_Nonfatal_Injuries_Tx_Hospital-ED_US2010-a.pdf (Accessed 21.9.2012)
|