A 68-year-old man with an underlying chronic obstructive pulmonary disease on a steroid inhaler presented with a one-month history of dysphonia. There was no dysphagia, odynophagia, neck swelling, or constitutional symptoms. There was also no choking, effortful speech, or shortness of breath. On examination, the patient appeared comfortable in the room air. Endoscopic laryngeal examination revealed whitish patches over the bilateral vocal cord with intact mobility [Figure 1]. Neck examination yielded unremarkable results.
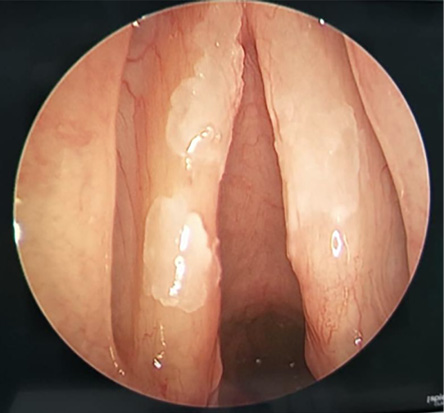 Figure 1: Endoscopic laryngeal examination revealed whitish patches on both vocal folds.
Figure 1: Endoscopic laryngeal examination revealed whitish patches on both vocal folds.
Question
What is the most likely diagnosis?
a. Laryngeal candidiasis.
b. Squamous cell carcinoma.
c. Chronic laryngitis.
d. Laryngeal tuberculosis.
Answer
a. Laryngeal candidiasis.
Discussion
Direct laryngoscopy and biopsy of the whitish lesion performed under general anesthesia revealed laryngeal thrush or candidiasis. The occurrence of laryngeal thrush was identified to be secondary to the steroid inhaler the patient was using. Therefore, the inhaler was withheld and the patient was prescribed daily oral fluconazole for two weeks. At one month follow-up, the hoarseness and vocal cord lesion had improved.
The term ‘thrush’ denotes a fungal infection involving mucous membranes following altered immunity. Common sites include the mouth, esophagus, and vagina. Isolated laryngeal thrush presenting with dysphonia is rare and is often a subject of diagnostic dilemma. Meticulous history taking is crucial, such as in this case, the usage of steroid inhaler. Although the fungus Candida is a part of the normal flora of laryngopharyngeal mucosa, altered immunity may result in superficial mucosal infection, notably upon chronic usage of both systemic and topical steroids, overzealous antibiotic usage, presence of neutropenia, as well as diabetes mellitus.
Other predisposing factors include radiotherapy, tissue trauma, reflux, and immune deficiency due to conditions such as AIDS. In the same vein, the literature describes cases of isolated laryngeal thrush presenting with dysphonia, cough, and signs of laryngeal irritation.1,2
The effectiveness of fluconazole in treating laryngeal thrush has been lauded following promising disease clearance. Additionally, it is crucial to identify and address the main causative factor for this condition by lowering the dosage and duration of steroid inhalers, utilization of spacer, or rinsing the mouth after spraying.3
Regarding the three incorrect answers, squamous cell carcinoma classically presents with a fungating mass over the glottic region. Chronic laryngitis results in inflammatory changes in the overall supraglottic structures. Laryngeal tuberculosis traditionally presents with an ulcerative lesion prominently over the interarytenoid region, arytenoid cartilages, posterior surface of true cords, and laryngeal surface of epiglottis, along with systemic manifestations such as loss of weight, loss of appetite, and night sweats.
references
- 1. Sulica L. Laryngeal thrush. Ann Otol Rhinol Laryngol 2005 May;114(5):369-375.
- 2. DelGaudio JM. Steroid inhaler laryngitis: dysphonia caused by inhaled fluticasone therapy. Arch Otolaryngol Head Neck Surg 2002 Jun;128(6):677-681.
- 3. Toogood JH. Inhaled steroid asthma treatment: ‘Primum non nocere’. Can Respir J 1998 Jul-Aug;5(Suppl A):50A-53A.