A growing preterm male infant was presented with fever and skin eruptions. He had been discharged a month earlier from the neonatal intensive care unit (NICU) after being born prematurely at 32 weeks of gestation (1250 grams, 3rd–5th centile) by emergency cesarean section done for maternal preeclampsia. He was fed by enteral routine throughout the four-week stay in the hospital. No prematurity-related ailments were seen in the infant, and he had an uneventful stay in the NICU. He was discharged home at physiological stability of 36 weeks post-menstrual age on kangaroo mother care, at a weight of 1850 grams with full enteral feeds supplemented with human milk fortifiers, iron, and vitamin D.
The infant presented at 40 weeks post-menstrual age and weighed 2400 grams. He was febrile (37.8 °C) but active and looked well. Skin eruptions were present all over the body except on oral mucosa and palms/soles. These lesions were in various stages of evolution, ranging from vesicles to blisters on erythematous macules approximately 1 cm in size. The vesicles and blisters were shiny and pink-to-red in color indicating underlying erythema and were filled with clear fluid. This appearance is often described as dew drops over rose petals. A few lesions had formed crusts. A Tzanck smear suggested multinucleated giant cells with ground glass nuclei on microscopy. There was no history of drug intake or similar lesions with fever within the family members. No contact with an infected person was reported at home, nor was there any community outbreak of febrile illness with similar rashes. No febrile illness with similar rashes was seen in other NICU graduates in the same hospital.
Our infectious disease specialist advised supportive treatment with antipyretics, topical emollients, oral acyclovir, and home isolation until all the lesions have crusted. During the follow-up visits, the infant had mild hyperpigmentation at the blister sites that faded over the next few weeks.
The infant was healthy at follow-up at four months of age.
Question
- What is the most likely diagnosis?
a. Monkeypox infection.
b. Community-acquired varicella-zoster infection.
c. Incontinentia pigmenti.
d. Perinatal varicella-zoster infection.
e. Miliaria crystallina.
Answer
b. Community-acquired varicella-zoster infection [Figure 1].
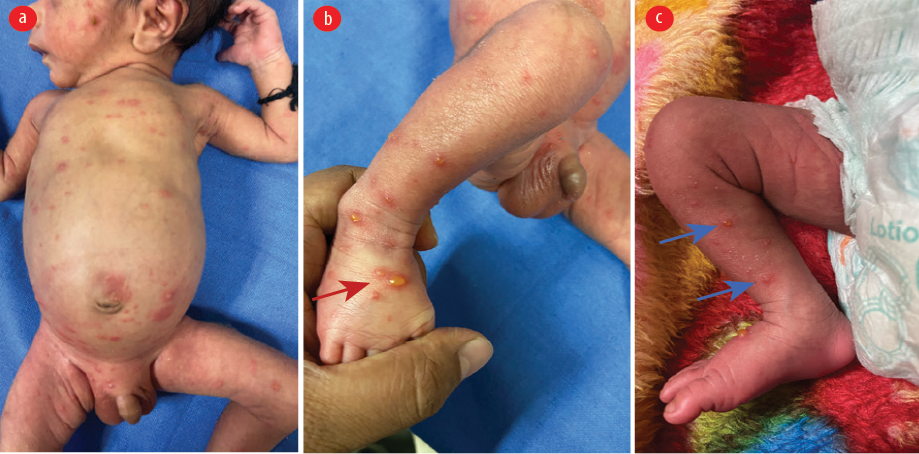 Figure 1: Dermatological manifestations of varicella-zoster infection in a growing preterm newborn. (a) Clear vesicles with underlying macules are present over the face, chest, abdomen, and acral parts described as dew drops on rose petals appearance. Lesions range from small fluid-filled vesicles to small bullae. (b) Bullous lesion with surrounding erythema (red arrow). (c) Typical dew-drops over erythematous base (blue arrows).
Figure 1: Dermatological manifestations of varicella-zoster infection in a growing preterm newborn. (a) Clear vesicles with underlying macules are present over the face, chest, abdomen, and acral parts described as dew drops on rose petals appearance. Lesions range from small fluid-filled vesicles to small bullae. (b) Bullous lesion with surrounding erythema (red arrow). (c) Typical dew-drops over erythematous base (blue arrows).
Discussion
Varicella-zoster infection is ubiquitous in tropical countries such as India. It can occur antenatally or postnatally in newborn infants. Early fetal infection may result in congenital varicella syndrome characterized by cicatricial skin lesions and various anomalies at birth. If the transmission occurs two days before delivery, it can result in a fulminant neonatal infection or disseminated infection with central nervous system symptoms. These two varieties of varicella-zoster infection can result in significant illness within a few days of birth.
The incubation period of varicella-zoster infection is usually 2–3 weeks. Infection in the current case was likely community-acquired, as the symptoms manifested after four weeks of discharge from the hospital. The diagnosis was made because of typical skin eruptions, positive Tzanck smear findings, and maternal-infant serology. A positive immunoglobulin G titer in the mother and positive immunoglobulin M titers in the infant suggested acute varicella-zoster transmission in the infant and supported the diagnosis of postnatal community-acquired viral transmission. The typical rashes evolved after 1–2 days of low-grade fever, which began over the face followed by other areas of sparing palms and soles. The simultaneous presence of pleomorphic rashes in various stages of evolution (vesicles, papules, and crusted lesions) differentiated it from other causes.
Community-acquired varicella-zoster infection in young preterm infants is uncommon and perplexing due to pleomorphic rashes and mild symptoms. The course of infection is usually favorable and with complete recovery; however, hospitalization may be required in severe cases. Therapy should be supportive and pragmatic.1 Our patient had a favorable outcome as seen in most cases of childhood varicella-zoster infection.
The differential diagnosis for the clear dew drops appearance of vesicobullous inflammatory dermatological conditions are rickettsial disease, neonatal syphilis, or monkeypox infection.2 Also, the absence of an erythematous macule with a clear dew drops appearance characterizes miliaria crystallina seen as sweat retention syndrome in hyperthermic conditions.3 Impetigo, a common skin infection in infants and children, also has an erythematous base but the content is purulent and yellow in contrast to the clear fluid seen in varicella-zoster infection. A positive polymerase chain reaction for varicella-zoster assay from the blister fluid can confirm the diagnosis.
The report illustrates an uncommon case of community-acquired varicella-zoster infection in a growing preterm-born infant in India. Its differentials are to be considered while evaluating vesiculobullous lesions in this population.
Disclosure
The authors declared no conflicts of interest. A written consent was given by the mother of the patient.
references
- 1. Blumental S, Lepage P. Management of varicella in neonates and infants. BMJ Paediatr Open 2019 May;3(1):e000433.
- 2. Sebaratnam DF, Minocha R, Fernández-Peñas P. Dermatology over the rainbow. JAMA Dermatol 2015 May;151(5):543.
- 3. Dimitrakoff J. Monkeypox virus infection across 16 countries - April-June 2022. N Engl J Med 2022 Dec;387(25):e69.