Cytomegalovirus (CMV) is a highly prevalent herpesvirus. CMV immuno-globulin G (IgG) positivity has been found to be 60% in the European population and as high as 90% in the Eastern Mediterranean Region (EMR) population.1,2 CMV causes prolonged latent infection and a wide spectrum of clinical presentations.3 In immunocompromised patients, it can cause significant morbidity and mortality. CMV infection is present in 60% of seropositive allo-hematopoietic stem cell transplant (HSCT) recipients, which can result in invasive end-organ diseases, such as enteritis and pneumonitis.4,5 Despite major advances in early diagnosis and management, seropositivity for CMV seems to be a risk factor for transplantation-related mortality in patients who receive a transplant from related donors.6
Current prevention strategies that utilize antiviral agents, such as ganciclovir or foscarnet, as preemptive therapy at the onset of viremia have sharply decreased the incidence of CMV end-organ diseases during the first three months after HSCT to 3–6% compared to 30% in the past.7–9 Generally, there is a preference for preemptive over prophylactic treatment, mainly due to the side effects of the available anti-CMV drugs.10 There is no consensus as to the cutoff CMV viral load for starting the preemptive therapy; however, it is typically initiated upon the first detection of CMV infection by a rapid detection method such as the pp65 antigenemia assay, pp67 messenger RNA assay, or DNA assay. Quantitative real-time polymerase chain reaction (PCR) assays for CMV DNA are increasingly preferred because of their high sensitivity and specificity and help monitor response to treatment. In the preemptive therapy strategy, all allogeneic HSCT recipients are monitored for CMV viral load every week till day 100 post-transplant.11
Internationally, the mortality rate of HSCT recipients due to CMV disease is very high, at nearly 46%.2 The corresponding figures for the EMR are lacking. HSCT service in Oman started in 1995 at Sultan Qaboos University Hospital (SQUH), Muscat. SQUH continues to be the only center in Oman offering the facility and performs allogeneic and autologous HSCT for 4–29 cases yearly. Due to limited bed availability, some patients are sent abroad to undergo the procedure.12
We aimed to estimate the incidence of CMV infection/disease in HSCT recipients during the first year post-transplant and investigate the risk factors for CMV infection as well as the clinical outcomes.
Methods
This was a retrospective observational cohort study of all allogenic HSCT recipients (n = 576) over 12 years (January 2006 to December 2018) who underwent the transplant either at SQUH or abroad and then were followed up at SQUH on their return (usually around day 30 post-transplant). Their one-year post-transplant medical history was collected. We excluded nine HSCT recipients who had CMV infection within three months prior to the transplant and eleven recipients whose records lacked regular CMV viral load testing data.
The patient records revealed that they were managed as per the following protocol adopted by SQUH: routine surveillance was conducted weekly for all HSCT recipients by testing plasma by CMV quantitative real-time PCR (COBAS AmpliPrep/COBAS TaqMan CMV test) for the first 100 days post-transplant and clinically indicated afterward. CMV infection was defined as the detection of viral nucleic acid in plasma. Recipients with CMV infection underwent enhanced surveillance by monitoring their CMV viral load twice weekly if preemptive therapy had not been started yet. CMV disease was identified if it met the case definition of proven or probable CMV disease: the presence of compatible symptoms or signs and CMV documentation by histopathology or detection of CMV DNA by real-time PCR in tissue from the affected organ or fluid based on the clinical scenario.12 Clinically significant CMV infection was considered CMV disease or CMV infection leading to preemptive therapy. The local CMV viral load cutoff to consider preemptive therapy was 500 copies/mL (454.5 IU/mL). However, preemptive therapy was started at any detectable CMV viral load for T-cell-depleted transplants.
We used t-tests and chi-square tests to compare nominal and ordinal variables between recipients with and without CMV infection. A multivariate logistic regression model was used to identify factors independently predictive of post-HSCT CMV infection. Kaplan-Meier and cumulative incidence estimation methods were used to estimate one-year overall mortality rates associated with CMV infection post-HSCT. Cox proportional hazard regression, providing hazard ratios, and 95% CI, were used to assess predictors of one-year overall mortality. A p-value ≤ 0.050 was considered statistically significant. All statistical analyses were conducted using IBM SPSS Statistics for Windows (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.).
Ethical approval was obtained from the medical research ethics committee at SQU on March 7, 2019 (Ref. MREC #1867/ 2019).
Results
The final subjects of this study were 556 HSCT recipients, of whom 308 (55.4%) were male. Their median age was 12 years with an interquartile range (IQR) of 5–22 years. Nearly two-thirds (366; 65.8%) had benign conditions such as beta thalassemia (24.8%), sickle cell disease (16.5%), aplastic anemia (4.3%), primary immunodeficiency (6.1%), and hemophagocytic lymphohistiocytosis (3.8%) [Table 1]. Malignant conditions were found in 190 (34.2%) participants, including acute lymphoblastic leukemia (15.5%), acute myeloid leukemia (12.6%), lymphoma (3.2%), and chronic myelogenous leukemia (2.9%). The vast majority (458; 82.4%) received their transplants from matched related donors. Myeloablative conditioning was given to 405 (81.2%) patients while reduced intensity conditioning (RIC) was given to 94 (18.8%). The median day of engraftment was day 13 (range = 2–33). Graft versus host disease (GVHD) was observed in 246 (44.2%) patients within one year post-transplant, among whom 115 (46.7%) had multiple organs involvement, while the rest had skin GVHD (62; 25.2%), gastrointestinal (41; 16.7%), or liver (18; 7.3%) involvement. CMV serostatus was not assessed in this study because it was documented only in 259 (46.6%) recipients (who had positive CMV immunoglobulin G ).
Table 1: Recipients’ demographic and clinical characteristics.
|
Age, years
|
|
|
|
< 12
|
276
|
49.6
|
|
≥ 12
|
280
|
50.4
|
|
Sex
|
|
|
|
Male
|
308
|
55.4
|
|
Female
|
248
|
44.6
|
|
Underlying disease
|
|
|
|
Beta thalassemia
|
138
|
24.8
|
|
SCD
|
92
|
16.5
|
|
ALL
|
86
|
15.5
|
|
AML
|
70
|
12.6
|
|
Lymphoma
|
18
|
3.2
|
|
HLH
|
21
|
3.8
|
|
Aplastic anemia
|
24
|
4.3
|
|
Fanconi anemia
|
17
|
3.1
|
|
Primary immunodeficiency
|
34
|
6.1
|
|
CML
|
16
|
2.9
|
|
Others*
|
40
|
7.2
|
|
HLA matching
|
|
|
|
Matched
|
458
|
88.2
|
|
Haploidentical
|
61
|
11.8
|
|
HSCT source
|
|
|
|
Bone marrow
|
138
|
27.6
|
|
PBSC
|
362
|
72.4
|
|
Conditioning regimen
|
|
|
|
Myeloablative
|
405
|
81.2
|
SCD: sickle cell disease; ALL: acute lymphoblastic leukemia; AML: acute myeloid leukemia; HLH: hemophagocytic lymphohistiocytosis; CML: chronic myelogenous leukemia; HLA: human leukocyte antigen; HSCT: hematopoietic stem cell transplant; PBSC: peripheral blood stem cells; RIC: reduced intensity conditioning.
*Other diseases present: myelodysplastic syndromes, multiple myeloma, neuroblastoma, osteopetrosis, paroxysmal nocturnal hemoglobinuria, hemoglobin S-Oman, epidermolysis bullosa, and bone marrow failure.
Out of the 556 recipients, 330 (59.4%; 95% CI: 55.200–63.400) experienced CMV infection within one year post-transplant, while the incidence of clinically significant CMV infection was 155 (27.9%; 95% CI: 24.200–31.600). CMV infection occurred at a median of 37 days after graft infusion (IQR = 24–56). The median CMV viral load at the time of the first detection of CMV infection was 150 copies/mL (IQR = 17–336 copies/mL). The median day of starting preemptive therapy was day 46 post-transplant. Ganciclovir was used as the initial agent in 97/155 (62.6%) recipients, valganciclovir in 37 (23.9%), and foscarnet in 18 (11.6%). The median time till the occurrence of viremia was longer (four weeks) in recipients who received preemptive therapy, and their median highest viral load reached 3313 copies/mL during the viremic phase. In contrast, among the recipients who did not receive preemptive therapy, the median time of viremia was shorter (two weeks) and their highest viral load was 150 copies/mL. The majority of 330 infected patients (261; 79.1%) had only one CMV infection episode during one year post-transplant.
Univariate and multivariate analyses were used to characterize the clinical variables that were associated with overall CMV infection and clinically significant CMV infection post-HSCT [Tables 2 and 3]. Univariate analysis of overall CMV infection showed a significantly increased risk of overall CMV infection with myeloablative conditioning compared to RIC (p = 0.002) and haploidentical donor versus human leukocyte antigen matched donor (p = 0.003). GVHD and age group ≥ 12 years (p < 0.001) were associated with a higher incidence of CMV infection. There was no evidence to support the increased risk of CMV infection in recipients receiving HSCT for malignancy (p = 0.102) versus benign disease or anti-thymocyte globulin based conditioning regimen (p = 0.580). Multivariate analysis further demonstrated a statistically significant relationship between overall CMV infection and myeloablative conditioning (odds ratio (OR) = 2.548, 95% CI: 1.480–4.388; p = 0.001), GVHD (OR = 1.721, 95% CI: 1.120–2.647; p = 0.013), haploidentical transplant (OR = 2.740, 95% CI: 1.342–5.587; p = 0.006), and age ≥ 12 years (OR = 3.155, 95% CI: 1.984–5.025; p < 0.001). Clinically significant CMV infection analysis showed similar results apart from the age variable failed to demonstrate clinically significant association in multivariate analysis [Table 3].
Table 2: Analysis of CMV infection (overall vs. clinically significant) among HSCT recipients.
|
Sex
|
|
|
|
|
|
Male
|
179 (58.1)
|
0.544
|
81 (26.4)
|
0.544
|
|
Female
|
151 (60.9)
|
|
74 (29.8)
|
|
|
Age, years
|
|
|
|
|
|
< 12
|
137 (49.6)
|
< 0.001
|
66 (23.9)
|
0.038
|
|
≥ 12
|
193 (68.9)
|
|
89 (31.9)
|
|
|
Underlying disease
|
|
|
|
|
|
Benign
|
208 (56.8)
|
0.102
|
95 (26.0)
|
0.195
|
|
Malignant
|
122 (64.2)
|
|
60 (31.6)
|
|
|
HLA matching
|
|
|
|
|
|
Matched
|
253 (55.2)
|
0.003
|
105 (23.0)
|
< 0.001
|
|
Haploidentical
|
46 (75.4)
|
|
36 (59.0)
|
|
|
Conditioning regimen
|
|
|
|
|
|
Myeloablative
|
256 (63.2)
|
0.002
|
124 (30.7)
|
0.002
|
|
RIC
|
43 (45.7)
|
|
14 (14.9)
|
|
|
ATG use
|
|
|
|
|
|
Yes
|
136 (58.4)
|
0.580
|
67 (28.8)
|
0.613
|
|
No
|
157 (61.1)
|
|
68 (26.6)
|
|
|
HSCT source
|
|
|
|
|
|
Bone marrow
|
72 (52.2)
|
0.025
|
25 (18.1)
|
0.001
|
|
PBSCT
|
229 (63.3)
|
|
117 (32.4)
|
|
|
GVHD
|
|
|
|
|
|
Yes
|
172 (69.9)
|
< 0.001
|
103 (41.9)
|
< 0.001
|
CMV: cytomegalovirus; HSCT: hematopoietic stem cell transplant; HLA: human leukocyte antigen; RIC: reduced intensity conditioning; ATG: anti-thymocyte globulin; PBSCT: peripheral blood stem cell transplantation; GVHD: graft versus host disease.
Table 3: Logistic regression of CMV infection risk factors among HSCT recipients.
|
Age, years
|
|
|
|
|
|
|
|
≥ 12 vs. < 12
|
3.155
|
1.984–5.025
|
< 0.001
|
0.614
|
0.988–2.681
|
0.056
|
|
HLA matching
|
|
|
|
|
|
|
|
Haploidentical vs. matched related
|
2.740
|
1.342–5.587
|
0.006
|
4.115
|
2.141–7.937
|
< 0.001
|
|
Conditioning regimen
|
|
|
|
|
|
|
|
Myeloablative vs. RIC
|
2.548
|
1.480–4.388
|
0.001
|
2.876
|
1.359–6.086
|
0.006
|
|
Underlying disease
|
|
|
|
|
|
|
|
Benign vs. malignant
|
0.696
|
0.434–1.115
|
0.132
|
0.722
|
0.433–1.204
|
0.212
|
|
HSCT source
|
|
|
|
|
|
|
|
BM vs. PBSCT
|
1.069
|
0.653–1.748
|
0.791
|
0.666
|
0.365–1.217
|
0.186
|
|
GVHD
|
|
|
|
|
|
|
CMV: cytomegalovirus, ; HSCT: hematopoietic stem cell transplant; OR: odds ratio; HLA: human leukocyte antigen; RIC: reduced intensity conditioning;
BM: bone marrow, PBSCT: peripheral blood stem cell transplantation; GVHD: graft versus host disease.
The incidence of CMV disease among the total study population was 1.8% (10; 95% CI: 0.690–2.900), and among those who had CMV infection, it was 3.0% (10; 95% CI: 1.200–4.800). Out of the 10 cases of CMV disease, five developed CMV pneumonitis, four had CMV colitis, and one developed CMV multisystem involvement (CMV pneumonitis, colitis, and retinitis). In the five recipients, CMV disease was confirmed by histopathology, while the other five were diagnosed with probable/possible CMV disease upon detection of CMV DNA in tissue/fluid. The median day for CMV disease was day 50 post-transplant (IQR = 35–195). The median initial viral load was 3547.5 copies/mL (IQR = 1812.8–4229.5), and the median duration of CMV viremia was six weeks. Ganciclovir was used for induction therapy for seven recipients, while three received foscarnet. For maintenance therapy, valganciclovir was used for eight recipients, while two continued on ganciclovir. The median duration of induction and maintenance therapy was two and three weeks, respectively. Ganciclovir resistance was confirmed by molecular testing in two recipients with CMV disease.
The overall one-year mortality was 8.3% (46; 95% CI: 6.000–10.600). CMV infection was associated with increased overall mortality (p = 0.001). Survival time was significantly lower among recipients with overall (p = 0.001) and clinically significant CMV infection (p < 0.001) compared to those free of CMV infection [Figure 1].
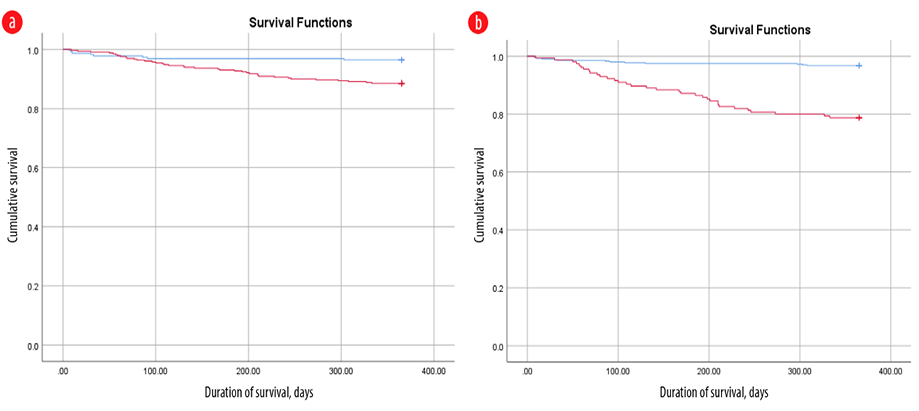 Figure 1: Comparative durations of survival for patients with (red line) and without cytomegalovirus (CMV) infection (blue line). CMV infection was associated with increased overall mortality (p = 0.001). (a) Survival time with all levels of CMV infection was significantly lower than without CMV infection (p = 0.001); (b) survival time with clinically significant CMV infection was significantly lower (p < 0.001) compared to those free of CMV infection.
Figure 1: Comparative durations of survival for patients with (red line) and without cytomegalovirus (CMV) infection (blue line). CMV infection was associated with increased overall mortality (p = 0.001). (a) Survival time with all levels of CMV infection was significantly lower than without CMV infection (p = 0.001); (b) survival time with clinically significant CMV infection was significantly lower (p < 0.001) compared to those free of CMV infection.
Discussion
To our knowledge, this is the largest cohort study of CMV infection post-HSCT in the EMR. The overall incidence of CMV infection in all allo-HSCT recipients in the current cohort was 59.3%, which was within the 39–60% range reported in the literature.13–15 However, the incidence of clinically significant CMV infection (i.e., CMV infection that required preemptive therapy or led to CMV disease) was 27.9%. The estimate of clinically significant CMV infection varies between institutions depending on which CMV viral load cutoff is used to initiate preemptive therapy. In one study, clinically significant CMV infection was reported at 59%, which is higher when compared to our finding that could be attributed to starting preemptive therapy at any detectable CMV level in that center.16
In our center, a CMV viral load of 500 copies/mL was taken as the cutoff to start preemptive therapy. The exceptions were T-cell-depleted recipients for those the therapy was started at any detectible CMV level. Since we had a good number (60.4%) of patients with highest detectable viral loads < 500 copies/mL, preemptive therapy was only given for 47.0% of CMV-infected recipients.
GVHD was a significant contributing factor for CMV infection in our study population, in line with several studies.12–14 Immunosuppressive effects of GVHD and its treatment play major roles in CMV replication. In addition, recipients who had a haploidentical transplant or received myeloablative conditioning were at higher risk of developing CMV infection than those who had human leukocyte antigen-matched transplants or received RIC. This might be attributed to administration of higher doses of myeloablative chemotherapy, leading to irreversible cytopenia and prolonging the recovery period of adaptive T-cell immunity.17 However, anti-thymocyte globulin use did not show any significant association between both groups.
In our cohort, older age was significantly associated with overall CMV infection (though not with clinically significant CMV infection), but studies elsewhere have varied in determining the role of age.14,15,18 For example, Sousa et al,14 and Lin et al,15 did not find the recipients’ age a significant risk factor for CMV infection. This might be attributed to the relatively higher age distribution in these studies. However, Takenaka et al,18 went in line with our finding that older age was an independent risk factor for CMV infection. This corresponds to an age-dependent rate of CMV seropositivity in the general population and different indications of HSCT among age groups where malignancy may be the major indication for HSCT in older recipients. In young recipients, the main indication would be hereditary blood diseases such as beta thalassemia and sickle cell disease, which accounted for most of our cohort due to high levels of consanguinity in the Omani population. We did not find a significant association between the prevalence of CMV infection and the nature of the underlying disease (malignant vs. benign) or the source of HSCT (bone marrow vs. peripheral blood stem cell).
The incidence of CMV disease in our one-year cohort post-transplant was 1.8%, much lower than the incidence of 8–16% reported in the literature.13,17,19 The risk of CMV disease in our cohort was low because of the strict CMV routine surveillance and the initiation of preemptive therapy at low-level viremia. On the other hand, a high CMV viral load was associated with an increased risk of CMV disease.13 We have also found that the overall one-year mortality in our cohort (8.3%) was much lower than the 30–61% rates reported in other studies.13,19 This can be explained by the age distribution and underlying disease, as the younger age group and benign primary diseases accounted for the majority of our cohort. However, overall mortality was higher among recipients with CMV infection, which could be a primary or a secondary outcome. CMV infection can also be attributed to multi-organ failure by cytopathic effect or a marker for illness severity.19
The major limitations of this study were its retrospective and observational nature, which prevented us from assessing the association between CMV serostatus and CMV infection due to missing data.
Conclusion
The incidence of CMV infection post-HSCT in this relatively young Omani cohort was comparable to the levels elsewhere, while those of CMV disease and overall mortality were lower. Older age, haploidentical transplant, myeloablative conditioning, and GVHD were significantly associated with a higher risk of CMV infection and with an increased risk of overall mortality in the first year post-transplant. Given the impact of CMV infection on HSCT recipients and the lack of consensus on the CMV level where preemptive therapy needs to be started, our findings support early initiation of preemptive therapy at low-level CMV viremia.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
Acknowledgments
We are grateful to the doctors and nurses at the bone marrow transplant unit of the hematology department, and the biomedical scientists at the microbiology and immunology department, SQUH.
references
- 1. Bazarbachi A, Labopin M, Ghavamzadeh A, Giebel S, Al-Zahrani H, Ladeb S, et al. Allogeneic matched-sibling hematopoietic cell transplantation for AML: comparable outcomes between Eastern Mediterranean (EMBMT) and European (EBMT) centers. Bone Marrow Transplant 2013 Aug;48(8):1065-1069.
- 2. Boeckh M, Leisenring W, Riddell SR, Bowden RA, Huang ML, Myerson D, et al. Late cytomegalovirus disease and mortality in recipients of allogeneic hematopoietic stem cell transplants: importance of viral load and T-cell immunity. Blood 2003 Jan;101(2):407-414.
- 3. Bhat V, Joshi A, Sarode R, Chavan P. Cytomegalovirus infection in the bone marrow transplant patient. World J Transplant 2015 Dec;5(4):287-291.
- 4. Boeckh M, Nichols WG. The impact of cytomegalovirus serostatus of donor and recipient before hematopoietic stem cell transplantation in the era of antiviral prophylaxis and preemptive therapy. Blood 2004 Mar;103(6):2003-2008.
- 5. Garrido RS, Aguado JM, Díaz-Pedroche C, Len O, Montejo M, Moreno A, et al. A review of critical periods for opportunistic infection in the new transplantation era. Transplantation 2006 Dec;82(11):1457-1462.
- 6. Broers AE, van Der Holt R, van Esser JW, Gratama JW, Henzen-Logmans S, Kuenen-Boumeester V, et al. Increased transplant-related morbidity and mortality in CMV-seropositive patients despite highly effective prevention of CMV disease after allogeneic T-cell-depleted stem cell transplantation. Blood 2000 Apr;95(7):2240-2245.
- 7. Marty FM, Ljungman P, Papanicolaou GA, Winston DJ, Chemaly RF, Strasfeld L, et al; Maribavir 1263-300 Clinical Study Group. Maribavir prophylaxis for prevention of cytomegalovirus disease in recipients of allogeneic stem-cell transplants: a phase 3, double-blind, placebo-controlled, randomised trial. Lancet Infect Dis 2011 Apr;11(4):284-292.
- 8. Chemaly RF, Ullmann AJ, Stoelben S, Richard MP, Bornhäuser M, Groth C, et al; AIC246 Study Team. Letermovir for cytomegalovirus prophylaxis in hematopoietic-cell transplantation. N Engl J Med 2014 May;370(19):1781-1789.
- 9. Azevedo LS, Pierrotti LC, Abdala E, Costa SF, Strabelli TM, Campos SV, et al. Cytomegalovirus infection in transplant recipients. Clinics 2015 Jul;70(7):515-523.
- 10. Boeckh M, Murphy WJ, Peggs KS. Recent advances in cytomegalovirus: an update on pharmacologic and cellular therapies. Biol Blood Marrow Transplant 2015 Jan;21(1):24-29.
- 11. Nichols WG, Price TH, Gooley T, Corey L, Boeckh M. Transfusion-transmitted cytomegalovirus infection after receipt of leukoreduced blood products. Blood 2003 May;101(10):4195-4200.
- 12. Al-Khabori M, Al-Huneini M. Hematopoietic stem cell transplantation in the Sultanate of Oman. Hematol Oncol Stem Cell Ther 2017 Dec;10(4):305-307.
- 13. Green ML, Leisenring W, Xie H, Mast TC, Cui Y, Sandmaier BM, et al. CMV viral load and mortality after hematopoietic cell transplantation: a cohort study in the era of preemptive therapy. Lancet Haematol 2016;3(3):e119-e127.
- 14. Sousa H, Boutolleau D, Ribeiro J, Teixeira AL, Pinho Vaz C, Campilho F, et al. Cytomegalovirus infection in patients who underwent allogeneic hematopoietic stem cell transplantation in Portugal: a five-year retrospective review. Biol Blood Marrow Transplant 2014 Dec;20(12):1958-1967.
- 15. Lin HC, Han SM, Hwang WL, Chou CW, Chang KH, Shi ZY, et al. Cytomegalovirus infection and treatment in allogeneic hematopoietic stem cell transplantation: a retrospective study from a single institution in an endemic area. Turk J Haematol 2017 Jun;34(2):159-166.
- 16. Ranti J, Perkonoja K, Kauko T, Korhonen R. Clinical and healthcare burden of disease associated with cytomegalovirus in allogeneic hematopoietic stem cell transplantation - a retrospective single-center study. Transpl Infect Dis 2022 Dec;24(6):e13947.
- 17. Rowe RG, Guo D, Lee M, Margossian S, London WB, Lehmann L. Cytomegalovirus infection in pediatric hematopoietic stem cell transplantation: risk factors for primary infection and cases of recurrent and late infection at a single center. Biol Blood Marrow Transplant 2016 Jul;22(7):1275-1283.
- 18. Takenaka K, Nishida T, Asano-Mori Y, Oshima K, Ohashi K, Mori T, et al. Cytomegalovirus reactivation after allogeneic hematopoietic stem cell transplantation is associated with a reduced risk of relapse in patients with acute myeloid leukemia who survived to day 100 after transplantation: the Japan society for hematopoietic cell transplantation transplantation-related complication working group. Biol Blood Marrow Transplant 2015 Nov;21(11):2008-2016.
- 19. Diaz L, Rosales J, Rosso F, Rosales M, Estacio M, Manzi E, et al. Cytomegalovirus disease in patients with hematopoietic stem cell transplantation, experience over 8 years. Hematol Transfus Cell Ther 2020;42(1):18-24.