|
Abstract
Primary liposarcomas of the female and male breasts are very rare. Heterologous differentiation in adipocytic tumors is also an exceedingly rare phenomenon, which is occasionally reported in the literature. We describe the case of a 22 year-old female who presented with a relatively large left breast mass which was clinically diagnosed as a case of giant fibroadenoma, but histologically showed a well differentiated liposarcoma with evidence of extensive chondroid differentiation. The mammographic and radiological features are presented and correlated with the histopathological appearances together with literature review and comparison with similar reported cases.
Keywords: Breast sarcomas; Liposarcoma; Chondroid/cartilaginous differentiation; Dedifferentiated liposarcoma.
Introduction
Although liposarcoma is considered to be one of the most common soft tissue sarcomas in adults, its occurrence in the breast is largely a curiosity. Dedifferentiated liposarcomas may occur in retroperitoneal sites but are very rare elsewhere. Dedifferentiated liposarcomas that contain low grade areas and cartilaginous differentiation have only been reported in association with myxoid liposarcoma. In such cases, the differential diagnosis involves phyllodes tumors and breast metaplastic carcinoma with chondroid differentiation.
Case report
A 22 year-old female was referred to the surgical unit because of a left breast mass. Clinical examination revealed a nodular left breast mass at the 4 O’clock position. The mass was approximately 8 cm in maximum diameter, slightly movable with overlying unremarkable but slightly "stretched" skin. The patient was married with two children and her past medical history was not significant. Her biochemical and hematology laboratory "work-up" was reported to be within normal limits. An initial clinical diagnosis of fibroadenoma was made. However, because of the atypical radiological picture, a decision to perform a tru-cut needle biopsy followed by excision was made.
Considering the patient’s young age, radiological assessment was initiated by an ultrasound breast study which showed a hypoechoic well encapsulated 6 × 3.7 cm mass at 4 O’clock location of the breast with multiple small internal cysts. Since the patient’s young age made a degenerating large fibroadenoma an unlikely possibility, an MRI was done for the patient. It showed the mass to be well-encapsulated with no parenchymal infiltration. It also demonstrated a rapidly enhancing capsule of the mass with internal heterogeneous content and gradual washout on post contrast T1WI (Fig. 1A). Fat suppression images showed only suppression of the peripheral part of the mass with non-suppressed multiple cystic internal components (Fig. 1B). What was clear from the MRI was that the mass was arising from the breast tissue itself and not the chest wall; however, the tissue characterization of the mass was non-specific.
The tru-cut biopsy from the described left breast lesion was reported as showing atypical chondroid tissue and a recommendation to provide an excision biopsy in order to exclude a diagnosis of sarcoma was made. The excision specimen consisted of a heterogeneous mass of partly fatty and partly firm glistening pale tissue measuring 8 × 5.5 × 4.5 cm. Histopathological examination revealed the presence of a low grade lipomatous neoplasm with extensive chondroid differentiation occupying more than 50% of the entire tumor volume (Figs. 2A and 2B). No epithelial component was identified in any of the many sections examined.
Immunohistochemical stains showed strong positivity of the tumor cells with both S100 protein and MDM 2 stains. A final diagnosis of primary low grade liposarcoma with extensive chondroid dedifferentiation was eventually made. The patient underwent a modified radical mastectomy operation with axillary clearance. She made an excellent post-operative recovery and remained well after 12 months of out-patient clinic follow-up.
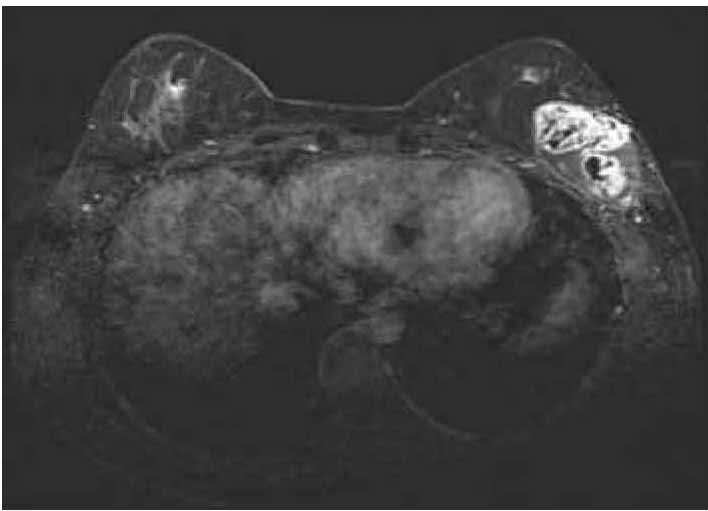
Figure 1A: Enhance capsule of the mass with internal heterogeneous content and gradual washout on post contrast T1WI.

Figure 1B: Suppression of the peripheral part of the mass with non-suppressed multiple cystic internal components.
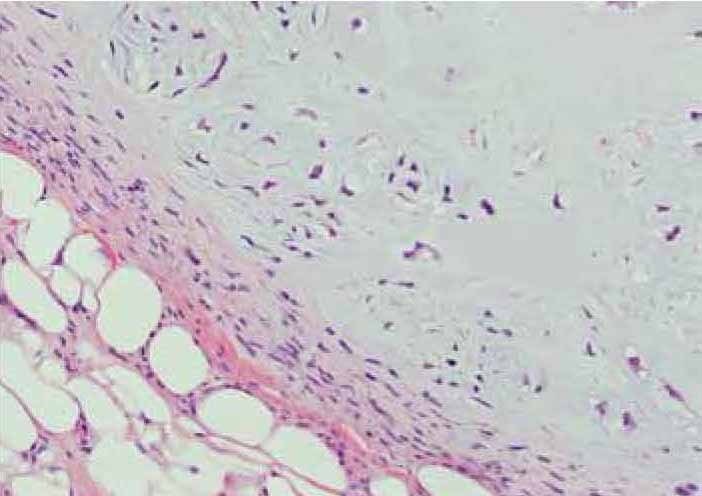
Figure 2A: Low grade liposarcoma of the breast (note the presence of the spindle cell and chondroid areas with "entrapped" lipocytes. The arrowhead points towards a lipoblast). Hematoxylin and Eosin stain × 200.
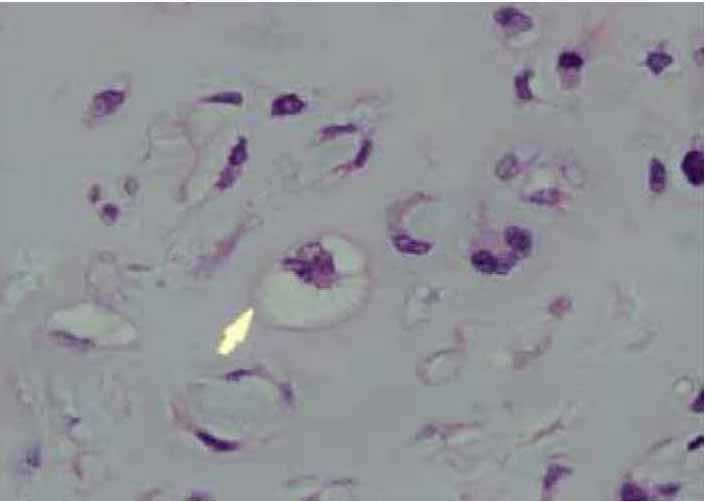
Figure 2B: Foci of atypical chondroid containing lipoblasts. Hematoxylin and Eosin stain × 400.
Discussion
Well differentiated liposarcoma is the most common form of this sarcoma, which can be encountered during adult life. In the collective experience of the Armed Forces Institute of Pathology and the Mayo Clinic (USA), 75% of cases developed in the deep muscles of the extremities and 20% in the retroperitoneum with the remainder divided between the groin, spermatic cord and other miscellaneous sites.1 Liposarcoma of the breast is a rare entity but has been reported in the literature.2-4
Dedifferentiation occurs in up to 10% of well differentiated liposarcomas and the risk of dedifferentiation appears to be higher when dealing with deep seated lesions, particularly the retroperitoneum.5 The concept of low grade dedifferentiation has increasingly been recognized.6 Furthermore, dedifferentiated liposarcoma may exhibit heterologous differentiation in about 5-10% of cases, which apparently does not affect the clinical outcome.5,6 Most often, the line of heterologous differentiation is myogenic or osteochondrosarcomatous, but other elements have also been reported.7
Primary sarcomas of the breast accounts for less than 1% of all breast malignancies.8 Cases of osteogenic sarcoma, chondrosarcoma, angiosarcoma, Leiomyosarcoma, malignant fibrous histiocytoma and neurogenic sarcoma have been reported in the literature.9-15
Our case represents a rare example of primary mammary low grade/well differentiated liposarcoma of the breast, which showed an unusual and almost unique extensive heterologous or divergent cartilaginous/chondroid differentiation. Literature search showed that this degree of low-grade dedifferentiation has not been reported in mammary carcinoma before. This feature of dedifferentiation is important to recognize, as dedifferentiated liposarcoma appears to exhibit less aggressive clinical behavior when compared with other high grade pleomorphic sarcomas.13-15
In cases of low grade dedifferentiated mammy sarcomas, as in our case, it is essential to rule out sarcomatous overgrowth of phyllodes tumors, sarcomatoid carcinoma and secondary sarcoma. The role of clinicopathological and radiologic correlation, immunohistochemistry and molecular genetics is, however, essential in this regard.
Conclusion
Well differentiated liposarcoma of the breast is a rare neoplasm. The possibility of chondroid dedifferentiation should be suspected if certain radiological features are present. However, confirmation will require adequate histopathological assessment and exclusion of malignant phyllodes tumors and sarcomatoid carcinoma.
Acknowledgements
The authors would like to express their gratitude to Ms. Maria Vivian C. Darusin for her excellent computer and secretarial skills during the typing of this manuscript.
References
1. Lucas DR, Nascimento AG, Sanjay BK, Rock MG. Well-differentiated liposarcoma. The Mayo Clinic experience with 58 cases. Am J Clin Pathol 1994 Nov;102(5):677-683.
2. Austin RM, Dupree WB. Liposarcoma of the breast: a clinicopathologic study of 20 cases. Hum Pathol 1986 Sep;17(9):906-913.
3. Pant I, Kaur G, Joshi SC, Khalid IA. Myxoid liposarcoma of the breast in a 25-year-old female as a diagnostic pitfall in fine needle aspiration cytology: report of a rare case. Diagn Cytopathol 2008 Sep;36(9):674-677.
4. Nandipati KC, Nerkar H, Satterfield J, Velagapudi M, Ruder U, Sung KJ. Pleomorphic liposarcoma of the breast mimicking breast abscess in a 19-year-old postpartum female: a case report and review of the literature. Breast J 2010 Sep-Oct;16(5):537-540.
5. Fletcher CDM (2000). Soft tissue tumours in: Diagnostic Histopathology of Tumours, Fletcher CDM, ed. 2nd ed. Churchill Livingstone: London.
6. Henricks WH, Chu YC, Goldblum JR, Weiss SW. Dedifferentiated liposarcoma: a clinicopathological analysis of 155 cases with a proposal for an expanded definition of dedifferentiation. Am J Surg Pathol 1997 Mar;21(3):271-281.
7. Wei YC, Li CF, Eng HL, Yeh MC, Lin CN, Huang HY. Myxoid liposarcoma with cartilaginous differentiation: identification of the same type II TLS-CHOP fusion gene transcript in both lipogenic and chondroid components. Appl Immunohistochem Mol Morphol 2007 Dec;15(4):477-480.
8. Barnes L, Pietruszka M. Sarcomas of the breast: a clinicopathologic analysis of ten cases. Cancer 1977 Oct;40(4):1577-1585.
9. De Medici A, Cebrelli CF, Venegoni A, Mottola P. [Primary osteogenic sarcoma of the breast. Clinical contribution]. Minerva Chir 1997 Nov;52(11):1375-1378.
10. Elemenoglou J, Zizi-Serbetzoglou A, Papatheofanis J, Nomikos IN. Primary osteogenic sarcoma of the breast. A case report. Eur J Gynaecol Oncol 1999;20(1):67-68.
11. Alaoui Slimani K, Allam W, Ichou M, Kettani F, Errihani H. Primary Chondrosarcoma Of The Breast: A Case Report . WebmedCentral BREAST 2010;1(9):WMC00553
12. Kirova YM, Feuilhade F, Calitchi E, Otmezguine Y, Le Bourgeois JP. Radiation-induced sarcomas following radiotherapy for breast cancer: six case reports and a review of the literature. Breast 1998;7:277-282 .
13. Székely E, Madaras L, Kulka J, Járay B, Nagy L. Leiomyosarcoma of the female breast. Pathol Oncol Res 2001;7(2):151-153.
14. Jones MW, Norris HJ, Wargotz ES, Weiss SW. Fibrosarcoma-malignant fibrous histiocytoma of the breast. A clinicopathological study of 32 cases. Am J Surg Pathol 1992 Jul;16(7):667-674.
15. Hauser H, Beham A, Steindorfer P, Schmidt F, Smola MG. Malignant schwannoma of the breast. Langenbecks Arch Chir 1995;380(6):350-353.
|