| |
Introduction
In recent times, malignant skin tumors have generated a lot of interest in dermatopathology and oncology research. This is attributed to the fact that skin cancer shows racial and geographic variation.1,2 Reports have shown that Australia has the highest incidence of primary skin cancer accounting for 80% of all skin malignancies.3-6 The lowest incidence rates of skin malignancies have been documented in Blacks and Asians.7 Previous Nigerian studies have documented that malignant skin cancers constituted 7% to 20% of all malignancies.2,7,8
There is a worldwide increase in the prevalence and mortality rate of skin cancer.3,8 This may be attributed to stratospheric ozone depletion resulting from burning of fossil fuels and atmospheric pollution. Again, technological advancement with resultant chronic exposure to radiation is furthermore implicated. Studies have shown that ultraviolet (UV) radiation, particularly UVB with wavelength of 290-320m is a major risk factor for malignant skin tumors.9,10 Skin carcinogenesis occurs in a multi-step process, in which the initial events leading to malignant transformation are yet to be unveiled. Other risk factors implicated in skin cancer etiology include chronic skin ulcer, chronic osteomyelitis and old scars.11
An increasing incidence of malignant skin tumors has been reported in Australia and USA. Though several studies have been done on malignant skin tumors in Nigeria, the exact prevalence in the country remains unknown. Significantly, there is a dearth of information on these cancers in University of Benin Teaching Hospital (UBTH). This study is thus aimed at defining the frequency and morphological patterns of malignant skin tumors at UBTH. Data derived from this study would be useful in the management of these lesions and moreover serve as baseline data for further research.
Methods
This retrospective study examined data of surgical biopsies from skin lesions received at the Department of Histopathology, University of Benin Teaching Hospital, (UBTH) Benin City, Edo State Nigeria, over a 25 year period from 1982 to 2007. The specimens were sent from the Departments of Dermatology and Surgery at UBTH and other hospitals within Benin City metropolis and neighboring states of Delta, Anambra, Bayelsa, Kogi and Ondo. The major sources of information were the surgical pathology register and duplicate copies of histology reports of all malignant skin tumors diagnosed within the study period.
All specimens sent for histology were fixed in 10% formalin solution, processed with Histokinette automated tissue processor, paraffin embedded, and sectioned at 3-5 microns using the microtome machine before staining with hematoxylin and eosin stains. The results obtained were analyzed with respect to age, sex and type of tumor. Special stains including Masson-Fontana was used where necessary. Malignant skin tumors were classified using the WHO classification of malignant skin tumors.12 Data analysis was performed using the SPSS version 16 statistical package.
Results
During the 25-year period of study, 694 skin specimens were received at the Pathology Department. Of these, 187 cases were malignant. Malignant skin tumors thus accounted for 27% of all skin lesions while benign skin tumors and non-neoplastic skin lesions accounted for 162 (23%) and 345 (49%) cases, respectively. Table 1 shows that the age range for all malignant skin tumors was 17-79 years with a peak incidence occurring in the 4th decade, accounting for 45 cases (24%). Of the 187 malignant cases, 109 (59%) were males while 78 (41%) were females with a male to female ratio of 1.4:1, with a mean age of 47 ± 3 years. The differences in the mean age among different types of skin malignancies were not found to be statistically significant (p>0.05).
Table 1: Distribution of histological types of malignant skin tumors.
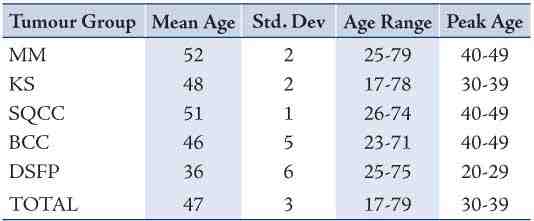
Table 2: Age and sex distribution of malignant skin tumors.
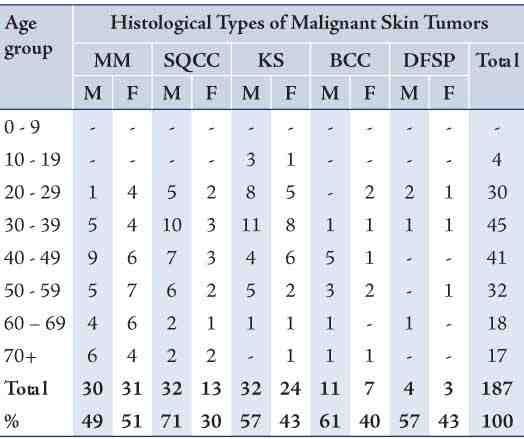
Table 3: Site distribution of malignant skin tumors.
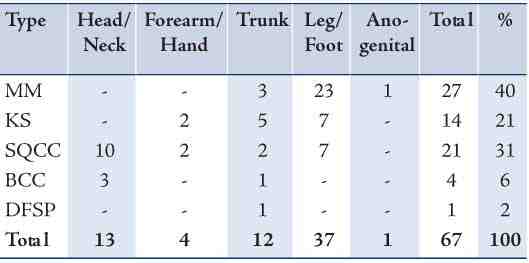
Figure 1: Trends of malignant skin tumors between1982 to 2008.
Table 3 shows the site distribution of malignant skin tumors. The majority of cases occurred in the leg and foot regions. Of the 67 cases with recorded site distribution (n=38; 57%), malignancy occurred in the leg and foot region. The trunk, head and neck regions were subsequently the most common sites accounting for 18% (n=12) and 17% (n=11), respectively. Only 5 cases (8%) occurred in the forearm and hand. There was a notable paucity of malignant skin tumors in the anogenital region as only 1 case (2%) was seen to have occurred at this site.
Malignant melanoma (MM) was the most common malignant skin tumor encountered in this study, constituting 61 cases (33%). Of these, 30 cases occurred in males while 31 cases occurred in females, giving a male to female ratio of 1:1.04 (p>0.05). The age range was 25-79 years and the peak age was in the 5th decade, while the mean age for MM was 52 ± 2 years (Tables 1 and 2). Of the 27 cases of malignant melanoma where recorded site distribution occurred in the leg and foot region 23 (85%), Kaposi sarcoma was the second most common malignant skin tumor encountered in this study, constituting 56 cases (30%). There was a slight male predominance with 32 cases occurring in males and 24 cases in females, giving a male to female ratio of 1.3:1 (p>0.05). The age range was 17-78 years and the peak incidence during the 4th decade, while the mean age was 46 ± 2 years (Tables 1 and 2). Only 14 cases of Kaposi sarcoma had records of site distribution. Seven (50%) occurred in the leg and foot region. Five out of the remaining 7 cases (36%) occurred in the trunk while 2 (14%) were seen in the anogenital regions. (Table 3)
Squamous cell carcinoma (SqCC) was the third most common malignant skin tumor encountered in this study, constituting 45 (24%) cases. The majority of these (32) cases occurred in males while 13 cases occurred in females, giving a male to female ratio of 3:1 (p<0.05). The age range and peak age at incidence were 26-74 years and 4th decades, respectively; with a mean age of 51 ± 1 years. The head and neck regions were the most common sites of occurrence for SqCC. Of the 21 cases of SqCC with recorded site distribution, 10 (48%) occurred in the head and neck regions. The leg and foot regions was the subsequent common sites accounting for 7 cases (33%) of SqCC. Basal cell carcinoma accounted for 18 cases (10%), with the majority in albinos (72% of cases), while the head and neck regions were the sites most commonly affected. There was a slight male predilection with 11 cases presented in males and 7 cases in females, giving a male to female ratio of 2:1 (p>0.05). The age range was from 23-71 years with a peak incidence in the 5th decade and a mean age of 46 ± 5 years. Dermatofibrosarcoma protuberans (DFSP) was rare and accounted for only 7 (4%) cases. The age range was 25-75 years with a peak in the 3rd decade and a mean age of 36 ± 6 years. Age had a significant effect on DFSP at (p<0.05) level of significance.
Discussion
In this study, malignant skin tumors constituted 6% of all malignancies. This is lower than the figure documented in the northern parts of Nigeria and India. Reports from Jos, Zaira, Kano and Maiduguri show that malignant skin tumors accounted for 7%, 12% 13% and 20% of all malignancies, respectively.2,7,8 A similar figure of 10% was reported in Yemen.13 It would appear however, that malignant skin lesions are rare in Asians, as rates as low as 1% and 1.4% have been documented in Pakistan and India, respectively.13,14 Notably, Australia has the highest documented incidence of skin cancer. This finding is partly attributed to its high altitude geographical location.5 The high incidence of malignant skin tumors in Caucasians has been attributed to the lower levels of onco-protective skin melanin which renders them more vulnerable to carcinogenic solar UV radiation, particularly from recreational sun exposure. Moreover, the risk is heightened by the current depletion of the ozone layer which normally filters UV radiation.
Malignant skin tumors accounted for 27% of all cutaneous lesions in Benin City; a figure, much higher than the 14% in Lagos reported by Keshinro.15 The frequency of malignant skin tumors particularly Kaposi sarcoma in UBTH, Benin City is generally on the increase. This is partly attributable to the increased prevalence and incidence of HIV and AIDS associated Kaposi’s sarcomas in Nigeria, sub-Saharan and all over the world. No reason can be attributable to the unstable increasing and decreasing frequency of malignant skin tumors over the 25-year study period at UBTH. (Fig. 1)
The age of patients is an important factor both for occurrence and management of skin malignancies. The current study findings show that the peak age of occurrence of malignant skin tumors was seen in the 4th and 5th decades. This is different from the report of Ochicha et al. in Kano, where the peak incidence of malignant skin tumors occurred in the 6th and 7th decades.2 The early peak age of malignant skin tumors observed in this study may be attributed to the early peak age incidence of Kaposi sarcoma occurring in the 4th decade of life. In this study, childhood malignant skin tumor was extremely rare. This was the same observation in Kano where no case was encountered.2 In this study, malignant skin tumors were slightly more prevalent in men with a male to female ratio of 1.4:1. A similar male to female ratio of 1.5:1 was documented by Keshinro in Lagos.15 Again, in Kano Ochicha et al. also observed a comparable male to female ratio of 1.2:1.2 The lower limb was the common site constituting 57% of cases.
A total of 61 cases of malignant melanoma (MM) were diagnosed, accounting for 33% of all malignant skin tumors. In Jos and Port Harcourt, malignant melanoma accounted for 25% and 39% of all malignant skin cancer, respectively. In this study, the mean age and peak age range were 52 years and the 5th decade, respectively. This corresponds with findings from the USA where the mean age was 53 years.16 The incidence of MM in Blacks is however, lower than in Caucasians. Most (85%) of the cases of MM in our study occurred in the leg and foot regions. This is consistent with reports from Kano, Maiduguri and Zaria (all in Northern Nigeria), where MM in the lower limb accounted for 70%, 86% and 93% of cases, respectively.7,8 In Eastern Nigeria, Onuigbo observed that MM mainly occurred on feet amongst Nigerians.17 Thus, MM seems to mostly occur in the feet of Africans as several studies conducted in Cameroon (West Africa), South Africa, as well as Kenya and Tanzania (East Africa) show the feet to be the most common site for malignant melanoma. However, it has been observed that in Caucasians, planter melanomas are far less common. Once more, reports from the USA show that MM occur relatively equally in both the lower limbs and trunk.18,19 This planter predilection of Negroid melanomas has prompted speculation of trauma and constant pressure on the weight bearing areas as possible etiological factors.2 This is quite different from Caucasians where UV radiation appears to be the major culprit, since the sun exposed parts of the body (head, trunk and legs) are the favorite sites.2,19 MM may also arise from melanotic nevus and hyperpigmented macules, with previous reports showing that melanocytic nevi and hyperpigmented macules are common on the plantar surface in Blacks.17,20
In this study, KS was the 2nd most prevalent skin malignancy accounting for 29.9% of malignant skin tumors. A study by Asuquo et al. reported KS to be the 2nd most common malignant skin tumor and constituting 33%, a figure similar to our report.15 However, our finding is higher than the 8%, 11% and 16% recorded in similar studies in Kano, Jos and Maiduguri, respectively.2,7 According to the 1999 national HIV sentinel survey, the north, north central and north east geographic zones where Kano, Jos and Maiduguri respectively belong have lower HIV infection rates of 2%, 7% and 5%, respectively. The reason for the increased incidence of KS in UBTH was as a result of rising prevalence of HIV infections. The mean age for KS was 48 years in this study. This report is at variance with findings from Togo, where the mean age was 35 years.
Our study at UBTH, Benin-City shows that SqCC was the third most common skin malignancy accounting for 25% of all malignancies. This contrasts with reports from other parts of Nigeria, Africa and America, where SqCC was the most common malignant skin tumor.2,7 In the USA, SqCC constitutes approximately 40% of all skin malignancies.21 However, the mean age for SqCC was 51 years in this study. This report is markedly different from findings recorded in Singapore, where the mean age was 84 years.21 No definitive reason was attributable to the marked variation in the mean ages. The head and neck were the most common sites of occurrence in our study. Indeed, this is similar to findings in other parts of the world. Studies have shown that SqCC and its variants normally follow an indolent course.22 This may be the reason why most African patients may not find it necessary to report to health facilities for proper assessment and therefore present late with advanced disease.
Basal cell carcinoma (BCC) accounted for only 10% of cases in this study, in marked contrast to the 70-80% reported in Caucasians.2 Again, studies conducted by Alakloby et al. in Saudi Arabia and other researchers in the Middle East show similar figures to what was obtained in the United States and Caucasian series.23 Furthermore, this is in contrast to our study and most African studies where BCC was a relatively rare finding. However, BCC seems to be relatively more common in our environment than most other parts of Nigeria as rates of 2%, 2%, 4% and 4% have been documented in Zaria, Maiduguri Jos and Kano, respectively.2,4,7,8 The mean age for BCC was 44 years in this study, which is at variance with the mean age of 55 years reported in the USA. BCC most commonly occurred in the head and neck regions with 75% of cases occurring AT these sites. This study finding is similar to other findings worldwide. In this study, BCC occurred predominantly in albinos, 13 out of the 18 cases occurred in albinos, thus accounting for 72% of all basal cell carcinomas.
DFSP was the least common malignant skin tumor recorded in this study, accounting for 4% of all malignant skin tumors at UBTH, Benin City. It most commonly occurred in the second and third decades of life with the overall male and female ratio of 1.3:1. This is comparable to reports in Kano,2 and Calabar.15 A rising incidence of all malignant skin tumors was observed. There was a striking increase in the incidence of Kaposi sarcoma between 2004 and 2008. While this may be part of the increasing incidence observed worldwide, a phenomenon partly blamed on the modern lifestyle of sexual promiscuity, it may also be partly attributed to the increasing incidence and awareness of HIV/AIDS in Nigeria. Finally the ongoing rise in skin cancer incidence calls for an urgent need to develop strategies for its prevention.
Conclusion
In this study, the majority of cases diagnosed as malignant skin tumor were seen in the 4th and 5th decades of life. Again, malignant melanoma was the most commonly diagnosed malignant skin cancer with high predilection for the leg and foot regions. Furthermore, a rising incidence of all malignant skin tumors was observed with Kaposi sarcoma in particular, confirming a remarkable increase from 2004-2008. This may be attributed to the increased prevalence and incidence of HIV in Nigeria, sub-Saharan Africa and other parts of the world. We advocate for adequate health education and screening with early presentation as a way to reduce the morbidity and mortality associated with malignant skin tumors in our environment.
Acknowledgements
The authors reported no conflict of interest and declare that this work was privately sponsored.
References
1. Mbuagbaw J, Pisoh C, Bengondo CM, Kegoum B, Takongmo S. Malignant Melanoma in Cameroon. Int J Surg 2007;9:1-6.
2. Ochicha O, Edino ST, Mohammed AZ, Umar AB. Dermatological Malignancies in Kano, Northern Nigeria. A histopathological review. Ann Afr Med 2004;3:188-191.
3. Jones RR. Ozone depletion and cancer risk. Lancet 1987 Aug;2(8556):443-446.
4. Boutwell WB. Under Cover: A community-based skin cancer prevention initiative. Cancer Bull 1993;45:279-281.
5. Borland RM, Hocking B, Godkin GA, Gibbs AF, Hill DJ. The impact of a skin cancer control education package for outdoor workers. Med J Aust 1991 May;154(10):686-688.
6. Rivers JK, Gallagher RP; Experience of the Canadian Dermatology Association. Public education projects in skin cancer. Cancer 1995 Jan;75(2)(Suppl):661-666.
7. Nggada HA, Na’aya HU, Ali NA. A Histological analysis of malignant tumours of the skin in University of Maiduguri Teaching Hospital, Nigeria. Highland Med Res J 2003;1:38-40.
8. Rafindadi AH, Samaila MO. Histopathologic analysis of epidermal skin tumours and tumour-like lesions in Ahmadu Bello University Teaching Hospital, Zaria. Niger Postgrad Med J 2006 Dec;13(4):354-356.
9. Williams IR, Kupper TS. Immunity at the surface: homeostatic mechanisms of the skin immune system. Life Sci 1996;58(18):1485-1507.
10. Johnson KO. The roles and functions of cutaneous mechanoreceptors. Curr Opin Neurobiol 2001 Aug;11(4):455-461.
11. Pearl DK, Scott EL. The anatomical distribution of skin cancers. Int J Epidemiol 1986 Dec;15(4):502-506.
12. Leboit PE, Burg G, Weedon D, Sarasin A. Pathology and genetics of tumours of the skin. IARC Press, Lyon 2004. 130-54.
13. Laishram RS, Banerjee A, Punyabati P, Sharma LD. Pattern of skin malignancies in Manipur, India. A 5 year histological review. J Pak Assoc Dermatol 2010;20:128-132.
14. Soomro FR, Bajaj DR, Pathan GM, Abbasi P, Hussain J, Abbasi SA. Cutaneous malignant Tumour. A profile of 10 years at LINAR, Larkana, Pakistan. J Pak Assoc Dermatol 2010;20:133-136.
15. Asuquo M, Umana A, Otei O, Bassey I, Ebughe G. Kaposi sarcoma in calabar, southern Nigeria. Oman Med J 2009 Jan;24(1):33-36.
16. Kricker A, Armstrong BK, English DR. Sun exposure and non-melanocytic skin cancer, cancer causes control 1994; 5: 367-92.
17. Onuigbo WI. Malignant melanoma in the Igbos of Nigeria. Br J Plast Surg 1975 Apr;28(2):114-117.
18. Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol 2002 Apr;146(Suppl 61):1-6.
19. Boni R, Schuster C, Nehrhoff B, Birg G. Epidemology of skin cancer. Neuroedocrinol let 2002; 22:48-51.
20. Greenlee RT, Murray T, Bolden S, Wingo PA. Cancer statistics, 2000. CA Cancer J Clin 2000 Jan-Feb;50(1):7-33.
21. Marks R. An overview of skin cancers. Incidence and causation. Cancer 1995 Jan;75(2)(Suppl):607-612.
22. Wani I. Metastatic squamous cell carcinoma of foot: case report. Oman Med J 2009 Jan;24(1):49-50.
23. Alakloby OM, Bukhari IA, Shawarby MA. Histopathological Pattern of Non-Melanoma Skin Cancer at King Fahd Hospital of the University in the Eastern Region of Saudi Arabia during the years 1983 to 2002. Cancer Ther 2008;6:303-306.
|
|