|
Abstract
Objectives: The prevalence of parental violence has been an area of major public concern. There are few available data detailing the ways parents and other caregivers discipline children, particularly in low and middle income countries. This study focuses on the prevalence of different types of maternal child abuse and its association with maternal anxiety in the socio-cultural context of Iran.
Methods: Participants in this cross-sectional study consisted of 562 mothers with the last child aged from 1 month to 12 years old who attended the Amirkola Children’s Referral Hospital in Mazandaran Province, Iran, seeking healthcare services for their children. Demographic characteristics of the mothers, their children and reactions to conflicts with children were evaluated by a validated version of Conflict Tactics Scale for Parent and Child. Also, the relationship between maternal anxiety and child abuse was assessed using the Spielberger State-Trait Anxiety Inventory. The association between variables was examined by Pearson correlation coefficient, independent t-test, one-way ANOVA, and multivariate regression.
Results: The prevalence of mother-to-child corporal punishment, severe physical abuse and very severe physical abuse were 436 (78%), 260 (46%) and 180 (32%), respectively. Verbal emotional abuse was reported by 506 (90%) participants and nonverbal emotional abuse was reported in 374 (67%) cases. A correlation was observed between child abuse and mothers’ age (p=0.02), as well as with the number of children in the family (p=0.03), and the mothers’ trait anxiety (p<0.001).
Conclusion: Overall, the assessment of maternal child abuse should be an important focus for evaluation in mothers with anxiety and vice versa, when child abuse is suspected, maternal psychological assessment should be essential.
Keywords: Anxiety; Child abuse; Maternal behavior.
Introduction
The term "family violence" encompasses a wide range of adverse dynamics perpetrated by a range of family members, referring most commonly to abuse or violence between husbands and wives, or parental abuse towards children.1 The behavior of adult parents arise from a variety of informal sources, including their own experiences during childhood, advice from grandparents; friends; medical providers as well as the community.2 Parental abusive behavior disrupts the child’s normal development,3-5 and bears negative outcomes.6-8 Mental and physical,9-11 as well as social and behavioral health problems are consequences of child abuse,12-14 which adversely affect the child’s long-term health-related quality of life.15
Researchers have shown that child abuse exists in all societies at varying degrees and forms. In a review of literature, 872,000 children were reported to be victims of child abuse or neglect in 2004 in the USA, and an estimated 1,490 children died in that same year due to abuse or neglect.16 The U.S. Child Protective Services also received a little over 2.5 million reports of child maltreatment in 2009, of which 61.9% were assigned for investigation.17 In a cross-sectional study on Chinese families, parents commonly used corporal punishment against their children.18 Notably, it has been reported that mothers were found twice as often as fathers to psychologically or physically abuse their children.19 However, this may be because they bear a larger share of parenting responsibilities in two-parent families.20
Although the Islamic Republic of Iran acceded to the Convention on the Rights of the Child (CRC) in 1993 and the Child Protection Law which was ratified by the Parliament of Iran in 2002 states that all kinds of abuse leading to physical, mental or moral damage to the child endangering their physical or mental health is prohibited (Article 2),21 some studies have reported different kinds of child abuse among Iranian children.22,23 It seemed that there are some challenges facing the education of parents, teachers and other significant figures in children’s lives, on the rights of children,24 thus the generation and dissemination of knowledge, raising public awareness, promotion of policy debate and mobilization of resources for the realization of the rights of children and youth are integral parts of the Country’s Program. In this way, the Ministries of Health and Education began to implement a National Communication Strategy to Prevent Child Abuse in 2004, and in 2007, a booklet titled ‘Disciplining Children with Kindness: A Shiite Shari’a Perspective’ presenting the views of several high-profile religious leaders on non-violent child education was provided by the UNICEF regional office in Iran.25
To the best of our knowledge, there are few (if any) studies that discussed the influence of family members, and these studies have not shown corporal punishment to be an aspect of maternal child abuse. Meanwhile, considering that maternal mental health status is a significant individual risk factor for maternal abusive behavior,26 and the fact that this issue has received very little attention to poor researches in an Iranian context; this study was thus performed to determine the multiple forms of maternal child abuse prevalent in Iran and their association with maternal anxiety.
Methods
In this cross-sectional study, different forms of child abuse in families were evaluated. Target respondents were mothers of children referred to the Amirkola Children’s Referral Hospital in Mazandaran Province, Northern Iran, for healthcare services for their children. The children were referred from all different cities within the province, besides the other provinces nearby. In this study, the participants were aged 18 years and older with their last child aged from 1 month to 12 years old. To avoid attributing the effects of children’s illness to maltreatment, if the mothers’ last child was the one who was admitted to this hospital, she was excluded from the study. All the participants completed a questionnaire after their children gained relative stability from illness.
In order to calculate the sample size, a mean prevalence of 50% for child abuse was considered, as shown in previous studies.27 With this prevalence, bearing the statistical error = 0.05 (which is an acceptable error), and the precise = 0.005, the sample size would then have to be at least 400. Since one of the considered objectives of this study was to assess child maltreatment in different age groups (from infancy to school age) and to include a sufficient sample to assess the relationship between some variables and child abuse, all eligible mothers (n = 562) who were referred within the specific period from January to December 2008 were included.
A demographic form was developed to seek the respondents’ personal information such as: mothers’ age, occupation and education, as well as their exposure to maltreatment during childhood. The number of children in the family, as well as the age and sex of the last child were assessed.
To determine prevalence of different types of maternal child abuse, a Persian version of Conflict Tactics Scale for Parent and Child (CTSPC) was used. The original version of this scale with an acceptable reliability (average: 0.70) was developed by Straus et al. to assess parental child abuse.28 It has been validated in some countries,29,30 and has been deemed acceptable for Iranian culture.31 This instrument was used to measure the frequency of abusive behaviors committed by the mother towards her last child during the past year. It consisted of 27 questions on abusive behaviors including physical aggression and emotional abuse.
Physical aggression included corporal punishment (3 questions), severe physical abuse (4 questions) and very severe physical abuse (4 questions). Corporal punishment was questioned as such: "spanked him/her on the bottom with your bare hand" and "pinched him/her". Severe physical abuse termed such as "slapped him/her on the face or head or ears" and "threatened him/her with a knife or gun." A clue to severe physical abuse incorporated acts such as "beaten him/her up, that is, hit him/her over" and "over as hard as you could and grabbed around the neck of the child".
Emotional abuse in the form of either verbal (5 questions) or non-verbal (11 questions) was used to measure verbal and symbolic acts by the parents intended to cause psychological pain or fear on parts of the child. An example of verbal emotional abuse was "swore or cursed at him/her" and "shouted, yelled or screamed at him/her." An example of non-verbal emotional abuse was "threatened to spank or hit him/her (with gesturing) but did not actually do it" and "took away privileges or isolated him/her."
Participants were asked to determine the times that they have used each kind of abusive behavior on their last child in the past year on a 6-point Likert scale (0 = never, 1 = it happened before last year, 2 = one to two times, 3 = three to five times, 4 = six to ten times, 5 = more than 10 times). The total score for each abusive behavior was the average score of its questions, meaning that the total score for physical aggression was the average score of its components (corporal punishment, severe and very severe physical abuse) and the total score of emotional abuse was the average score of its components (verbal and non-verbal). In this regard, the total score of maternal child abuse was the score of physical aggression plus emotional abuse score. Also, to report the frequency of maternal child abuse, respondents who reported one or more instances of each abusive behavior during the last year, against the referent cases who reported none, were considered as a positive history of child maltreatment.
To assess the correlation between maternal child abuse and mothers’ anxiety, the trait component of Spielberger State-Trait Anxiety Inventory was used.27 It is a 20 item self-administered instrument which is widely used and extensively validated (Cronbach’s α = 0.94).32 Each item is scored on a 4-point Likert scale (from 1 = not at all, 4 = very much), with minimum and maximum overall scores varying from 20 to 80. The 75th percentile was used as thresholds to indicate high levels of anxiety.33
The collected data were fed into the Statistical Package for Social Sciences for Windows version 13.0 (SPSS Inc., Chicago, IL, USA) for further analysis. Descriptive statistics were used to determine maternal and child demographic characteristics and frequency of all kinds of maternal child abuse. The relationship between variables was evaluated by Pearson correlation coefficient, independent t-test, one-way ANOVA, and multivariate regression model. A p-value of 0.05 or less was considered statistically significant.
All mothers were informed about the purposes and methods of the study. They were informed that participation in the study was voluntary. Moreover, they were reassured that their responses would be kept confidential and their identities would not be revealed in research reports or in published findings. Finally, informed consent was obtained from each individual who agreed to participate in the study. This study was approved by Ethical Committee of Mazandaran and Babol Universities of Medical sciences.
Results
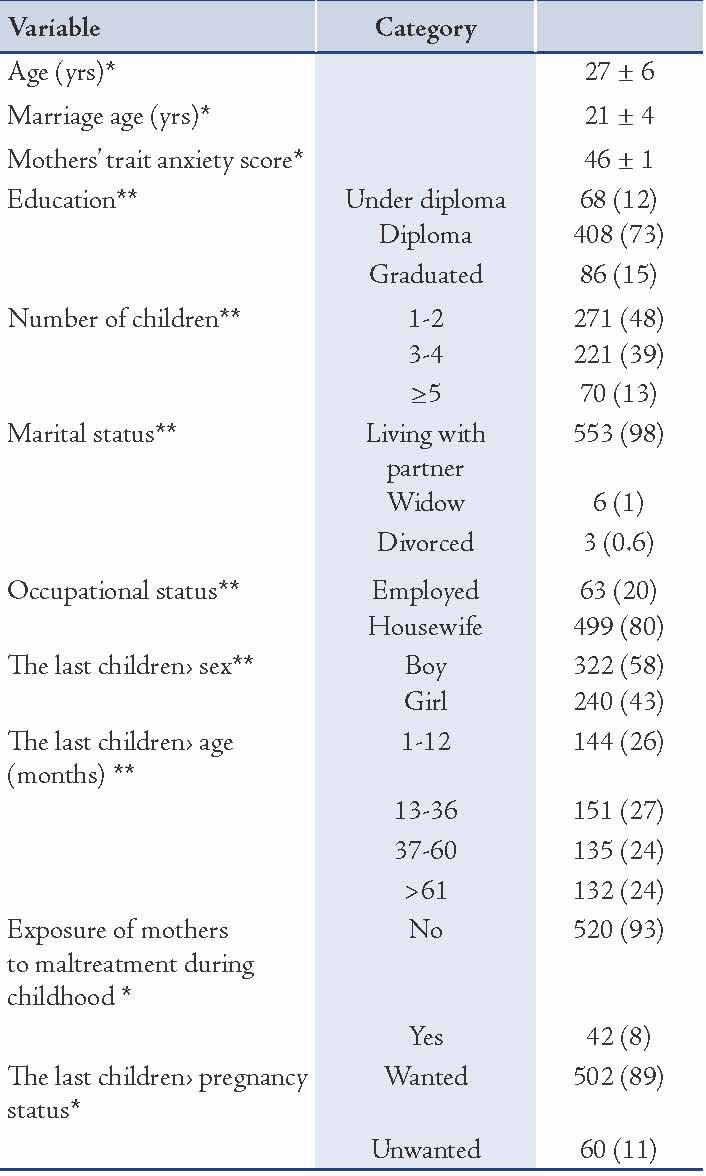
From the results, the age of the respondents ranged from 18 to 36 years (27 ± 6) and the mean age at marriage was 21 ± 4 years. The demographic characteristics of participants are shown in Table 1.
Table 1: Demographic characteristics of the participants.
The results showed that 92% of the participants perpetrated at least one of the abusive behaviors on their children during the last year. The frequencies of all types of abusive behaviors are detailed in Table 2. In general, results showed that a large number of mothers (436; 78%) had committed corporal punishment and the most frequent form of abuse was encountered among 365 (65%) participants who responded with the affirmative to the notion of "Spanked him/her on the bottom with your bare hand". Among the severe physical abusive behaviors, "slap on the face or head or ears" was the most common form to be reported (170; 30%), and the most common form of very severe physical abuse was "beat him/her up, that is, you hit him/her over and over as hard as you could" with 98 (18%) participants responding with the affirmative. In terms of verbal and non-verbal emotional abuse, "shouted, yelled or screamed" and "I don’t like you" were the most frequent forms reported with (407; 72%) and (323; 58%), respectively.
Univariate analysis showed that a relationship existed between maternal child abuse score and mothers’ age (r=0.13; p<0.001), mothers’ marital status (p=0.04), the number of children in the family (r=0.21; p<0.001), mothers’ exposure to maltreatment during childhood (p=0.03), unwanted pregnancy (r=0.41; p=0.05) and mothers’ trait anxiety score (r=0.48; p<0.001). One-way analysis revealed a mean score of maternal child abuse in mothers with pre-school and school aged children to be more than in other groups (p<0.001). (Table 3)
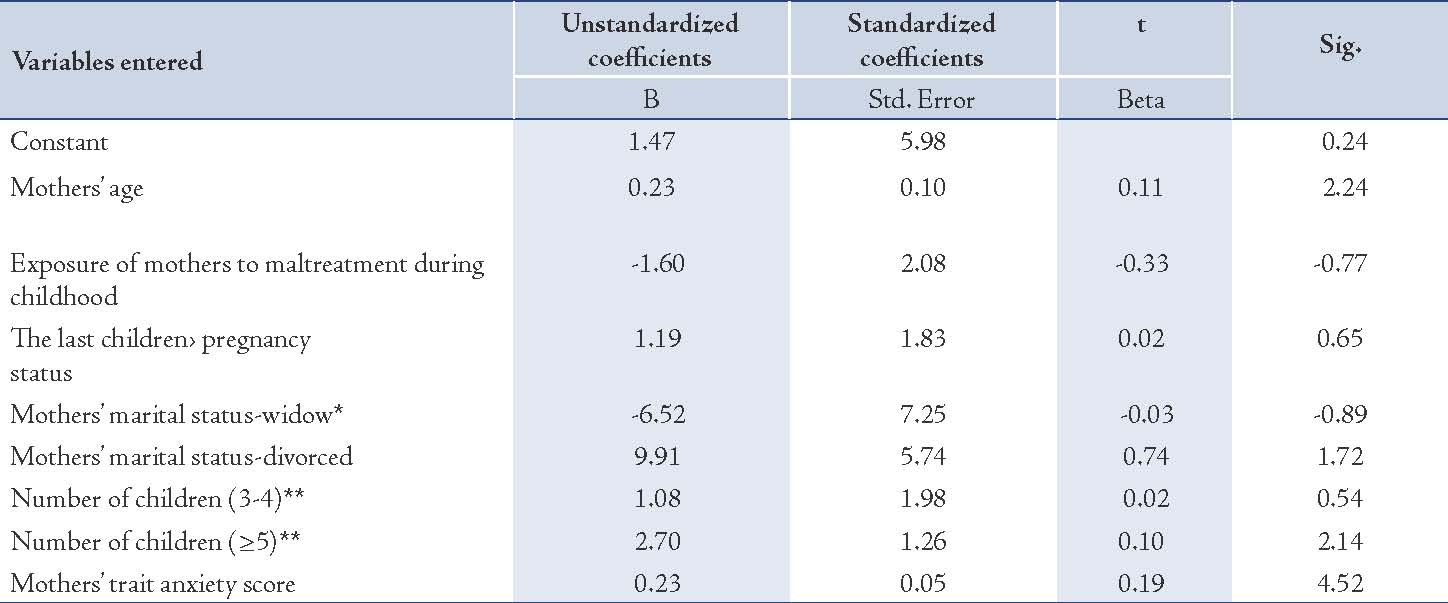
The results from multivariate regression analysis suggest a meaningful relationship between maternal child abuse with mother’s age and the number of children in the family. Interestingly, mothers with a higher trait anxiety score exhibited significantly higher mean score of abusive behaviors. (Table 4)
Table 2: Frequency and percentage of any kind of maternal-child abuse.
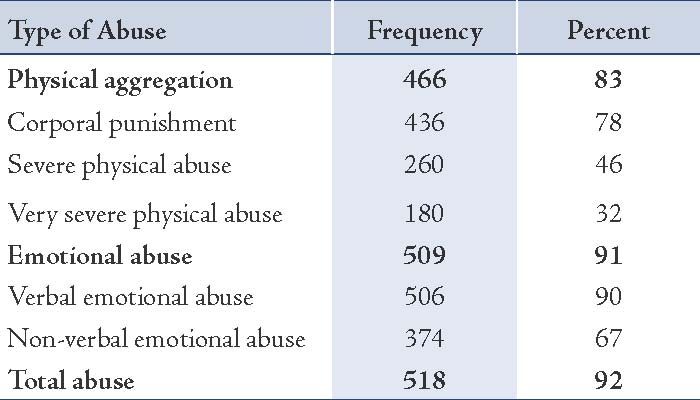
Table 3: Anova analysis of total abuse score in different age groups of children.
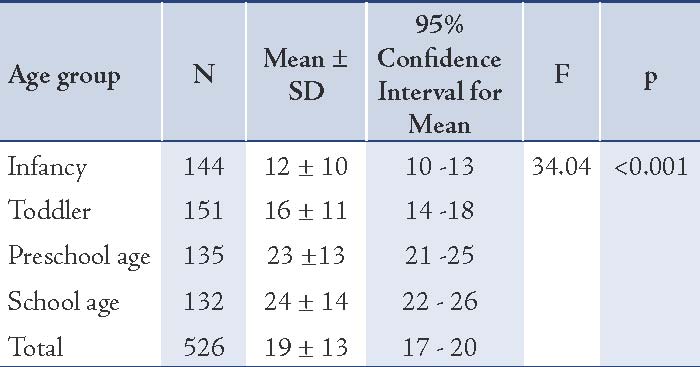
Table 4: Multiple regression between entered variables and maternal-child abuse score.
Discussion
This study is one of the first investigations conducted in the socio-cultural context of Iran assessing the link between maternal mental health status and child abuse. Violence of any kind has been a major health problem, but crimes against children are perhaps the hardest to comprehend. As little is understood about the factors associated with child maltreatment in developing countries and in order to design and implement support services and promote health status of these innocent victims in the world, including Iran, it is essential to conduct more studies to determine the various aspects of child abuse.
The results from the current study showed that a great proportion of the respondents had committed an act of verbal emotional abuse. In a longitudinal study conducted in the USA, verbal assertion was used more commonly than other misbehaviors.34 While in a study conducted by Malik, he argued that children were most commonly emotionally /psychologically abused rather than physically abused.35 Also, consistent with other researches,18,36 this study demonstrated that many mothers had attempted corporal punishment. Actually, parents were willing to disclose their use of corporal punishment because they think corporal punishment is necessary for nurturing the child and enforcing discipline.
Results from this study provides evidence against the generalization of very severe physical abuse, in contrast to the findings of a study conducted in a Kurdistan province by Stephenson et al.23 This difference may have been as a result of a larger sample size used in this study. Also, it is noted that in the present study, participants were referred to a referral center from surrounding provinces with different cultures. Thus, this study may provide a more accurate finding and could broaden our knowledge of maternal child abusive behaviors in the Iranian context.
The current study revealed a mean score of abuse in mothers with school and pre-school aged children to be more than in mothers with children of the other age groups. Previous researches have also shown that childhood maltreatment was common.34,35 This may arise as a result of family conflicts that can cause maternal harsh discipline. However, some mothers perceive children to be more responsible for their harsh treatment, perhaps as a consequence to endorse harsher punishment.37 Thus it would seem fair to suggest that in order to reduce maltreatment of preschool and school aged children, it is important to educate and maintain the concepts and definition of physical abuse and how to disclose acts of abuse. To generalize these concepts to actual abusive situations, a school-based prevention program in addition to an intensive media program would be very useful.38
The current study findings indicated an association between maternal age and child abuse. It is probable that older mothers have more children than younger mothers and they are more likely sustained for abusive behavior. Although it has been reported that evidence supporting the association between parental age and abusive behavior was not consistent so as to provide clear conclusions.39
As with previous studies, our results showed an association between the number of children in a family and maternal child abuse.39,40 Large families are not only significantly associated with the risk of physical abuse, but they also bear the risk of recurrence of child abuse.40,41 This is probably because with the increasing number of children in the family, parents have less time and energy to monitor and discipline each child and may use child abusive tendencies as a prompt behavioral controlling mechanism. This is more manifested when large families are faced with economic burdens to meet economic demands of their children.
This study also showed that maternal child abuse was associated with maternal anxiety. Luthor and Sexton reported that parental stress was linked with children’s lifetime limit setting, closeness with children’s externalizing problems and every day competences.42 Considering that anxiety is more frequent in females compared with males,3 and the fact that higher percentage of mental disorders among married Iranian women than married men, this may have in fact arisen as a result of patriarchy in the Iranian population, especially among lower social class populations.43 However, an important step towards management of maternal anxiety is to promote mothers to pay more attention to their children and spend more time with them. In general, the results from this study support the need for intervention and prevention programs to minimize child abuse.
The limitations in this study include the fact that this study only enrolled mothers with a child not exceeding the age of 12 years, because this age range (1 month - 12 years) was supposed to match the age limit of pediatric patients. Thus the inclusion of children up to the age of 18 years, would not have fully encompassed the CRC definition of a child, and would have resulted in an overall decreased rate of maltreatment among the sample. In addition, from each family, only mothers participated in our study, and it is likely that if fathers or other caregivers were also included, occurrences of all types of child abuse would have been judged differently. Finally, in this study, child abuse was assessed based on self-reported questionnaires, which may not be as accurate as direct real life observation based on certain situations under natural conditions.
Conclusion
Overall, maternal stress demonstrates a clear direct role in physical abuse. Such findings as those observed in this study suggest that targeting mothers’ sense of control and stress in relation to their immediate social environment holds particular potential to reduce the risk of physical abuse. In this way, assessment of child maltreatment should be an important focus of evaluation in mothers with anxiety and when child abuse is suspected, thus maternal psychological assessment should be essential. It is suggested that a well-designed study should be conducted to assess the management of maternal stress and its impact on minimizing child abuse to further strengthen the current findings. Also, a call for more studies to investigate other forms of child maltreatment like child neglect, which may be different from child physical abuse and deserves its own investigation as to the cause and treatment is recommended. Research of the impacts of abusive and neglectful fathers should be a topic for future studies.
Acknowledgements
We thank all the respondents who participated in this study. This study was sponsored by Mazandaran University of Medical Sciences (Grant Number: 85-60). The authors report no conflicts of interest.
References
1. McCloskey LA, Eisler R. Family Structure and Family Violence. Encyclopedia of Violence, Peace & Conflict 2008:813-820.
2. Fernandopulle S, Fernando D. Development and initial validation of a scale to measure emotional abuse among school children aged 13-15 years in Sri Lanka. Child Abuse Negl 2003 Oct;27(10):1087-1099.
3. Conroy E, Degenhardt L, Mattick RP, Nelson EC. Child maltreatment as a risk factor for opioid dependence: Comparison of family characteristics and type and severity of child maltreatment with a matched control group. Child Abuse Negl 2009 Jun;33(6):343-352.
4. Taussig HN, Culhane SE. Emotional maltreatment and psychosocial functioning in preadolescent youth placed in out-of-home care. J Aggress Maltreat Trauma 2010 Jan;19(1):52-74.
5. Sylvestre A, Mérette C. Language delay in severely neglected children: a cumulative or specific effect of risk factors? Child Abuse Negl 2010 Jun;34(6):414-428.
6. Berzenski SR, Yates TM. Classes and consequences of multiple maltreatment: a person-centered analysis. Child Maltreat 2011 Nov;16(4):250-261.
7. Topitzes J, Mersky JP, Reynolds AJ. From child maltreatment to violent offending: an examination of mixed-gender and gender-specific models. J Interpers Violence 2012 Aug;27(12):2322-2347.
8. Toth SL, Manly JT. Bridging research and practice: challenges and successes in implementing evidence-based preventive intervention strategies for child maltreatment. Child Abuse Negl 2011 Aug;35(8):633-636.
9. Rogosch FA, Dackis MN, Cicchetti D. Child maltreatment and allostatic load: consequences for physical and mental health in children from low-income families. Dev Psychopathol 2011 Nov;23(4):1107-1124.
10. Christian CW, Schwarz DF. Child maltreatment and the transition to adult-based medical and mental health care. Pediatrics 2011 Jan;127(1):139-145.
11. Tanaka M, Wekerle C, Schmuck ML, Paglia-Boak A; MAP Research Team. The linkages among childhood maltreatment, adolescent mental health, and self-compassion in child welfare adolescents. Child Abuse Negl 2011 Oct;35(10):887-898.
12. Bennett DS, Sullivan MW, Lewis M. Young children’s adjustment as a function of maltreatment, shame, and anger. Child Maltreat 2005 Nov;10(4):311-323.
13. Milot T, Éthier LS, St-Laurent D, Provost MA. The role of trauma symptoms in the development of behavioral problems in maltreated preschoolers. Child Abuse Negl 2010 Apr;34(4):225-234.
14. Garrido EF, Culhane SE, Raviv T, Taussig HN. Does community violence exposure predict trauma symptoms in a sample of maltreated youth in foster care? Violence Vict 2010;25(6):755-769.
15. Draper B, Pfaff JJ, Pirkis J, Snowdon J, Lautenschlager NT, Wilson I, et al; Depression and Early Prevention of Suicide in General Practice Study Group. Long-term effects of childhood abuse on the quality of life and health of older people: results from the Depression and Early Prevention of Suicide in General Practice Project. J Am Geriatr Soc 2008 Feb;56(2):262-271.
16. U.S. Department of Health and Human Services AoC, Youth and Families: Child Maltreatment 2004. Washington DC: US Government Printing Office 2006.
17. Child Protective services Avilable at. http://enwikipediaorg/wiki/Child_Protective_Services#cite_note-40.
18. Tang CS. Corporal punishment and physical maltreatment against children: a community study on Chinese parents in Hong Kong. Child Abuse Negl 2006 Aug;30(8):893-907.
19. Wilcox WB, Dew J. Protectors or perpetrators? Fathers, mothers, and child abuse and neglect. Research Brief No 7 AmericanValuesorg, http://wwwamericanvaluesorg/pdfs/researchbrief7pdf 2008.
20. Sapi MC, Vasconcelos JS, Silva FG, Damião R, Silva EA. Assessment of domestic violence against children and adolescents with enuresis. J Pediatr (Rio J) 2009 Sep-Oct;85(5):433-437.
21. Child Protection Law Available at:wwwlawyaleedu//iran_child_prot_law_engpdf.
22. Tavakol K, Azimi S, Sharifirad G, Hoseini A. Attitude change toward child abuse after educating behavioral intention model to mothers referred to Falavarjan health homes in 2007-2008. Journal of Research in Behavioural Sciences 2008;6(1):37-44.
23. Sheikhattari P, Stephenson R, Assasi N, Eftekhar H, Zamani Q, Maleki B, et al. Child maltreatment among school children in the Kurdistan Province, Iran. Child Abuse Negl 2006 Mar;30(3):231-245.
24. Ziaei S, Abedi HA, Arbaban M. Situation of children’s rights in Isfahan city. Iran J Nurs Midwifery Res 2011;16(2):141-147.
25. Unicef: Child disciplinary practices at home: Evidence from a range of low and middleincome countries. United Nations Children’s Fund Statistics and Monitoring Section Division of Policy and Practice 3 UN Plaza New York, New York 10017, USA.
26. Shin DW, Stein MA. Maternal depression predicts maternal use of corporal punishment in children with attention-deficit/hyperactivity disorder. Yonsei Med J 2008 Aug;49(4):573-580.
27. Stith SM, Liu T, Davies LC, Boykin EL, Alder MC, Harris JM, et al. Risk factors in child maltreatment: A meta-analytic review of the literature. Aggress Violent Behav 2009;14(1):13-29 .
28. Straus MA. Bibliography of the revised Conflict Tactics Scales (CTS2) and the Parent-Child Conflict Tactics Scales (CTSPC). World Health 2006;82(5):330-337.
29. Reichenheim ME, Moraes CL. Psychometric properties of the Portuguese version of the Conflict Tactics Scales: Parent-child Version (CTSPC) used to identify child abuse. Cad Saude Publica 2006 Mar;22(3):503-515.
30. de Zoysa P, Rajapakse L, Newcombe PA. Adaptation and validation of the parent-child conflict tactics scale for use in Sri Lanka. Ceylon Med J 2005 Mar;50(1):11-14.
31. Aeen F, Deris F, Shahgholian N. Different kinds of child abuse and it’s diposing factors. Iranian Journal of Nursing Reasearch 2001;14(28):47-54.
32. Spielberger CD, Vagg PR. Psychometric properties of the STAI: a reply to Ramanaiah, Franzen, and Schill. J Pers Assess 1984 Feb;48(1):95-97.
33. Dayan J, Creveuil C, Herlicoviez M, Herbel C, Baranger E, Savoye C, et al. Role of anxiety and depression in the onset of spontaneous preterm labor. Am J Epidemiol 2002 Feb;155(4):293-301.
34. Hussey JM, Chang JJ, Kotch JB. Child maltreatment in the United States: prevalence, risk factors, and adolescent health consequences. Pediatrics 2006 Sep;118(3):933-942.
35. Malik F. Determinants of child abuse in Pakistani families: Parental acceptance-rejection and demographic variables. International Journal of Business and Social Science 2010;1(1):67-80.
36. Alyahri A, Goodman R. Harsh corporal punishment of Yemeni children: occurrence, type and associations. Child Abuse Negl 2008 Aug;32(8):766-773.
37. Mitchell SJ, Lewin A, Horn IB, Rasmussen A, Sanders-Phillips K, Valentine D, et al. Violence exposure and the association between young African American mothers’ discipline and child problem behavior. Academic pediatrics 2009; 9(3):157-163.
38. Kaplan SJ, Pelcovitz D, Labruna V. Child and adolescent abuse and neglect research: a review of the past 10 years. Part I: Physical and emotional abuse and neglect. J Am Acad Child Adolesc Psychiatry 1999 Oct;38(10):1214-1222.
39. Fuhua Zhai, Qin Gao. Child maltreatment among Asian Americans: characteristics and explanatory framework. Child Maltreat 2009 May;14(2):207-224.
40. Kim J. Type-specific intergenerational transmission of neglectful and physically abusive parenting behaviors among young parents. Child Youth Serv Rev 2009;31(7):761-767 .
41. Bae H, Solomon PL, Gelles RJ. Multiple child maltreatment recurrence relative to single recurrence and no recurrence. Child Youth Serv Rev 2009;31(6):617-624 .
42. Luthar SS, Sexton CC, Abidin R, Adams C, Drabman R, Bargee J, et al. Maternal drug abuse versus maternal depression: vulnerability and resilience among school-age and adolescent offspring. Dev Psychopathol 2007;19(1):205-225.
43. Ghaleiha A, Afzali S, Bazyar M, Khorsand F, Torabian S. Characteristics of hospitalized patients following suicide attempt in hamadan district, iran. Oman Med J 2012 Jul;27(4):304-309.
|