| |
Abstract
Behcet’s disease is a multi-systemic inflammatory disorder with cutaneous acneiform eruptions, orogenital aphthae, uveitis, arthritis and systemic vascular inflammation. One of the rare vascular manifestations is thoraco-abdominal aortic and pulmonary aneurysm that is associated with high risk of morbidity and mortality. We report a 36-year-old man with chronic cough, hemoptysis, significant weight loss, and orogenital ulcers from one year before referral. Initial assessments revealed multiple parahillar nodules in chest X-ray, chronic inflammatory anemia, erythrocyte sedimentation rate more than 100, and positive Human Leukocyte Antigen B5 and B51. Evaluation for infection and malignancies was unremarkable. Open exploratory lung study showed multiple pulsatile nodules in both lungs. AMIGO computed tomogram confirmed multiple right and left pulmonary artery aneurysms and impending to rupture aneurysm at subdivision of inferior mesenteric artery. After beginning of three methylprednisolone and cyclophosphamide pulse doses, the clinical aspect of the patient dramatically improved. Although pulmonary aneurysm is a rare manifestation of Behcet’s disease and it is more infrequent in the distal branches, it can be seen in patients presenting with inflammatory disease and respiratory manifestations and with Behcet’s disease diagnosis. Corticosteroid pulse-therapy could be considered as the first line of medical treatment in these patients.
Keywords: Behcet’s disease; Aneurysm; Pulmonary Artery; Inferior mesentric artery; Medical treatment.
Introduction
Behcet’s disease (BD) is an autoimmune disorder with multi-systemic involvement. Clinical aspect of the patient occurred as pseudofolliculitis on the skin, uveitis, arteritis, orogenital aphthous ulcers and vascular involvement.1,2 Behcet’s disease (BD) is an inflammatory disorder with an unknown cause.3 Behcet’s disease diagnosis, according to the criteria of International Study Group, is based on recurrent oral ulcers and at least two of the disorders including uveitis, skin pseudofolliculitis, positive pathergy test and recurrent genital ulcers.4,5 BD is distributed endemically along the ancient silk route from Mediterranean countries to Eastern Asian countries. Its highest prevalence is reported from Antalya, Turkey with 370 patients per 100,000 inhabitants, whereas in northern European and North and South American countries, BD is a rather rare disorder. In Iran, the prevalence is reported as 68 patients per 100,000 population.6,7 A rare vascular manifestation of these patients is pulmonary artery aneurysm that affects mainly the young men presenting with hemoptysis, chest pain, cough and dyspnea, and is associated with poor prognosis.8 According to the previous studies, prevalence of vascular manifestations is between 5% to 32%.9,10 The most related predictor of this disease morbidity and mortality is arterial aneurysm.11,12 The most common sites of aneurysmal involvement are as follows: Pulmonary arteries, thoracic and infrarenal segments of aorta, carotid, subclavian, femoral and popliteal arteries. Distal vessels involvement and complications are very infrequent.12
Case Report
A 36-year-old man with chronic cough and hemoptysis with significant weight loss was admitted to the Internal Medicine Ward in Qaem hospital, Mashhad. The patient also complained of malaise, chills, night sweating and intermittent painful genital and oral aphthous ulcerations. Signs of systemic inflammation besides with low grade fever, pallor, orogenital ulcers, acneiform eruptions on the skin were seen on physical examination. Rhonchi and crackles were heard in both lungs but wheezing was not detected.
Chest X-ray revealed multiple right and left parahilar nodules without pleural effusion markings (Fig. 1). Tuberculosis and malignant lymphadenopathy were considered as the differential diagnoses. All of the laboratory analyses for infection or tuberculosis were negative. Except for erythrocyte sedimentation rate (more than 100 mm/hr), inflammatory anemia, and positive HLA-B5 and HLA-B51, other findings including C-ANCA, P-ANCA, ANA, circulating lupus-anticoagulant antibody, C3, C4 and CH50 were in normal range. PPD and pathergy skin test after 48-72 hours were not reactive. Slit lamp examination for uveitis was normal. During the three-week hospitalization, bloody paroxysmal cough of the patient continued without response to the supportive therapy. Bronchoscopy showed the normal views and bronchoalveolar lavage analysis was not accompanied with malignant changes. High resonance computed tomography (HRCT) of lungs revealed multiple left and right parahilar conglomerate masses (2 cm × 2 cm) with parenchymal fibrotic bands in the left lower lobe. Informed consent for open lung biopsy was obtained. Prominent pulmonary arteries surrounded with adhesions due to fibrotic tissues, and multiple pulsatile masses in both lungs were reported in open lung biopsy through sternotomy. Cytopathologic study of lung tissue biopsy showed necrosis and intimal fibroplasia of arteries that was associated with lymphocytic vasculitis and numerous intra-alveolar hemosideromacrophage without malignant changes.
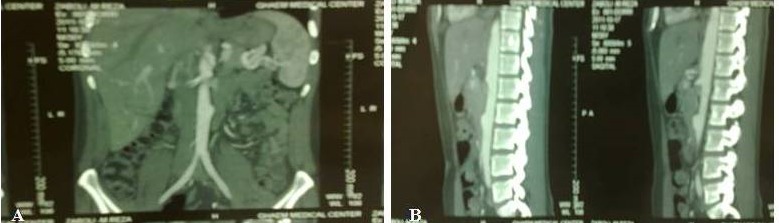
Figure 1: Multiple parahillum masses (A) and Multiple Bilateral pulmonary aneurysm (B).
Aortic and pulmonary CT-angiography showed fusiform aneurysmal changes in the left (35 mm) and saccular changes (16 mm) in the right pulmonary arteries, besides impending to rupture aneurysm at the subdivision of inferior mesenteric artery (Fig. 2). Although pathergy test was negative and the patient had normal examination for uveitis and arthritis, the diagnosis of Behcet’s disease was established.

Figure 2: Nipple of aneurysm, Impending to rupture (A) and Subdivision of inferior mesenteric artery aneurysm (B).
The patient was treated initially with 3 doses of methylprednisolone (30 mg/kg/day) for three days as a pulse therapy and followed by cyclophosphamide (750 mg/m2/mo), then prednisolone (1 mg/kg/day) were administrated and tapered through 2 weeks. One week later, dramatic disappearance of bloody sputum, cough and marked regression of signs and symptoms of inflammatory disease were observed. ESR fell from 105 mm/hr to 40 mm/hr. After four weeks of the medical treatment, ESR decreased to 4 mm/hr, CXR was cleared, cough and hemoptysis were stopped and the patient had better general appearance without any change in the pulmonary and abdominal aneurysms. Two weeks later after referring him to the surgery ward, the patient died suddenly due to the rupture of inferior mesenteric artery aneurysm.
Discussion
Some studies reported the prevalence of vascular injury in Behcet’s disease is 32%, that 80% of them were venous and 20% of them has been associated with arterial system involvement.13,14 Arterial aneurysm, venous and arterial occlusions are three types of histopathologic patterns of Behcet’s vasculitis.12,15-18
Although pulmonary artery vasculitis is infrequent and pulmonary artery aneurysm is very rare, the thoraco- abdominal aorta and the pulmonary artery are the most common sites of involvement accompanied with high rate of morbidity and mortality.17-19 Despite usual manifestations of pulmonary aneurysm, our patient had multiple bilateral aneurysms in the distal branches of the right and left pulmonary arteries which is very rare. The time usually needed for pulmonary manifestations of Behcet’s disease appearance is approximately 3.6 years after other extrapulmonary signs and symptoms. However, according to some studies, there is usually undetermined time between the diagnosis of Behcet’s disease and beginning of aneurysmal manifestations.13,14,20,21
Takir et al. reported that Helical Computed Tomography (HCT) is the method of choice for detecting aneurysm, since excellent vascular imaging could be provided by a small quantity of contrast material.21 Recently non-contrast MRA is preferred because of its contrast imaging study, but potentially increases the risk of complications like thrombus and aneurysm formation due to catheterization or rupture of aneurysm by rapid injection of large quantity of contrast media.17,22,23
Chance of aneurysmal rupture in Behcet’s disease is not always related to the size of the aneurysm; whereas, delay in the treatment has more important role.11 For this reason, early diagnosis and treatment of pulmonary aneurysm is associated significantly with decreased rate of morbidity and mortality.24 Hamuryudan et al. reported that the survival rate of patients with pulmonary aneurysm was 62%.25 ESR and chest X-ray are the best factors for evaluation of pulmonary aneurysm and response to treatment.12,26
There are two policy for treatment of Behcet’s disease with aneurysmal manifestations; surgical and medical managements.11 In acute phase, the surgical operation is not recommended due to the increased rate of thrombosis and suture dehiscence.10 The cornerstone of its treatment is administration of corticosteroid as a pulse therapy followed by corticosteroid and cyclophosphamide with or without anticoagulant drugs as maintenance treatment.
Some studies showed that anti-TNFα antibody (infliximab, adalimumab), azathioprine or colchicine plus corticosteooids had been tried successfully for the remission of aneurysm and inflammatory manifestations.2,26-28 Arterial embolism is the third policy for the treatment of patients with multiple aneurysms.24
Conclusion
Although pulmonary aneurysm is a rare manifestation of Behcet’s disease, and it is more infrequent in the distal branches, but it might be seen in patients presented with pulmonary and inflammatory disease manifestations, and with Behcet’s disease diagnosis. Corticosteroid pulse-therapy could be considered as the first line of medical treatment in these patients.
Acknowledgments
The authors reported no conflict of interests and no funding was received for this work.
References
1. Saba D, Saricaoğlu H, Bayram AS, Erdoğan C, Dilek K, Gebitekin C, et al. Arterial Lesion in Behcet’s disease. Vasa 2003;32(2):75-81 .
2. Baki K, Villiger PM, Jenni D, Meyer T, Beer JH. Behcet’s disease with Lite- Threatening haemoptoe and pulmonary aneurisms: complete remission after infliximab treatment. Ann Rheum Dis 2006;65(11):1531-1532 .
3. Alpagut U. ugurlucan M, Dayioglu E. Major arterial involvement and review of Behcet’s disease. Ann Vasc Surg 2007;21:232-239 .
4. Kasirajan K, Marked JM, Langsfeld M. Behcet’s disease: Endovascular management of a ruptured peripheral arterial aneurism. J Vasc Surg 2001;34:1127-1129 .
5. Aktoğu S, Erer OF, Urpek G, Soy O, Tibet G. Multiple pulmonary Arterial aneurism in Behcet’s disease: clinical and radiologic remission affer cyclophophamide and corticosteroid therapy. Respiration 2002;69:168-1810.
6. Davatch IF, Jamshid IA, Tehrani A, et al. Prevalence of Behcet’s disease in Iran: a WHO-ILAR: COPCORD stage I study. APLAR J Rheumatol 2007;10(3):239-243 .
7. Kaneko F, Nakamura K, Sato M, Tojo M, Zheng X, Zhang J. Epidemiology of Behçetís Disease in Asian Countries and Japan. Adv Exp Med Biol 2004;528:25-29 .
8. Criteria for diagnosis of Behçet’s disease. International Study Group for Behçet’s Disease. Lancet 1990;335:1078-1080. Anonymous.
9. Kuzu MA, Ozaslan C, Köksoy C, Gürler A, Tüzüner A. Vascular involvement in Behcet’s disease: 8 year-audit. World J Surg 1994;18:948-953 .
10. Alpagut U, Ugurlucan M, Dayioglu E. Major arterial involvement and review of Behcet’s disease. Ann Vasc Surg 2007;21:232-239 .
11. Rico JV, Pedrajas FG, González IC, Segura Iglesias RJ. Urgent endovascular treatment of a ruptured tibioproneal pseudoaneurism in Behcet’s disease. Ann Vasc Surg 2011;25(3):384-386 .
12. Kasirajan K, Marked JM, Langsfeld M. Behcet’s disease: Endovascular management of a ruptured peripheral arterial aneurism. J Vasc Surg 2001;34:1127-1129 .
13. Kim WH, Choi D, Kim JS, Ko YG, Jang Y, Shim WH. Effectiveness and safety of endovascular aneurysm treatment in patients with vasculo-Behçet disease. J Endovasc Ther 2009 Oct;16(5):631-636 .
14. Iscan ZH. Vural Km, Bayazit M. Compelling nature of arterial manifestation in Behcet’s disease. J Vasc Surg 2005;41(1):53-58 .
15. Erkan F, Cavadar T. Pulmonary vascuhitis in Behcet’s disease. Am Rev Respir Dis 1992;146(1):232-239 .
16. Roguin A, Edoute Y, Milo S, Shtiwi S, Markiewicz W, Reisner SA. A fatal case of Behcet’s disease associated with muitiple cardiovascwar lesion. Int J Cardiol 1997;59:257-273 .
17. Mouas H, Lortholary O, Lacombe P, Cohen P, Bourezak SE, Deloche A, et al. Embolization of multiple pulmonary arterial aneurism in Behcet’s disease. Scand J Rheumatol 1996;25:58-60 .
18. Numan F, Islak C, Berkmen T, Tüzün H, Cokyüksel O. Behcet’s disease: pulmonary arterial involvement in is cases. Radiology 1994;162:456-468.
19. Ben Ghorbel I, Ibn Elhadj Z, Khanfir M, Houman MH. Pulmonary arterial aneurysms in Behçet’s syndrome. Report of 4 cases. Arch Mal Coeur Vaiss 2004;97(12):1195-1199.
20. Trombati N, Souabny A, Aichane A, Bahlaoui A, Afif H, Bouayad Z. Pulmonary arterial aneurysms revealing Behçet’s disease: from diagnosis to treatment. Rev Med Interne 2002;23:334-341 .
21. El Houari T, Oukerraj L, Ghzaiel L, Fellat I, Azeroual M, Serraj K, et al. Management of Behcet’s disease with Multiple complication. Hellenic J Cardiol 2009;50(5):420-422.
22. Berlman T. MR. MR angiography of aneurysms in Behçet disease: a report of four cases. J Comput Assist Tomogr 1998;22(2):202-206 .
23. Tunaci A, Berkmen YM, Gökmen E. Thoracic involvement in Behcet’s disease: pathologic, clinical, and image feature. AJR Am J Roentgenol 1995;164(1):51-56 .
24. Kasikcioglu E, Akhan H, Cuhadaroglu C, Erkan F. Pulmonary artery aneurysm in Behcet’s disease: a case report. Heart Vessels 2004;19(3):157-159 .
25. Kwon Koo B, Shim WH, Yoon YS, Kwon Lee B, Choi D, Jang Y, et al. Endovascular therapy combined with immunosuppressive treatment for pseudoaneurysms in patients with Behçet’s disease. J Endovasc Ther 2003;10(1):75-80 .
26. Lee SW, Lee SY, Kim KN, Jung JK, Chung WT. Adalimumab treatment for life threatening pulmonary artery aneurysm in Behçet disease: a case report. Clin Rheumatol 2010;29(1):91-93 .
27. Gotor MA, Medrano J, Ruiz C, Alfonso ER, Guerrero J, de Gregorio MA. Pulmonary artery aneurysm and thrombosis caused by vasculitis in Behçet’s disease. Arch Bronconeumol 1997 Dec;33(11):591-593.
28. Vivante A, Bujanover Y, Jacobson J, Padeh S, Berkun Y. Intracardiac thrombus and pulmonary aneurysms in an adolescent with Behçet disease. Rheumatol Int 2009;29(5):575-577.
|