|
Abstract
Objective: To investigate antibiotics prescribing patterns in the outpatient pediatric emergency clinic at Queen Rania Al Abdullah II Children’s Hospital at Royal Medical Services in Amman, Jordan.
Methods: The data was collected from the emergency pharmacy over the period of a -five consecutive months. The methodology recommended by the World Health Organization for investigating drug use in a health facility was followed. The study measures the percentage of encounter with a prescribed antibiotic and the percentage share of each antibiotic category. The distribution of diagnostic categories that accounted for all antibiotics being prescribed and the distribution of each antibiotic being prescribed for upper respiratory tract infections (URTIs) were also measured.
Results: Antibiotic prescribing was frequent during pediatric visits to the outpatient pediatric emergency clinic resulting in a high percentage of encounters (85%) when compared to appropriate. Emergency physicians continue to frequently prescribe broad spectrum antibiotics which accounted for approximately (60%) of the total prescribed antibiotics and (83%) of prescribed antibiotics for upper respiratory tract infections and macrolides (primarily azithromycin) were the leading class among them.
Conclusion: Our results showed high consumption of antibiotics by emergency department pediatricians which highlight the importance for interventions to promote rational and judicious prescribing. An insight into factors influencing antibiotics prescribing patterns by military prescribers is required.
Keywords: Antibiotics; Prescribing patterns; Children; Military prescribers; Rational use.
Introduction
Antibiotics were found to be the most commonly prescribed and used categories of drugs in several national and international studies.1 In spite of their effectiveness to treat many bacterial infections, they are frequently used inappropriately to treat viral infections as in many cases of upper respiratory tract infections (URTIs).2 Such practice with no clinical benefit will increase the load of chronic diseases, develop bacterial resistance, elevate cost of health services and develop many side effects.2-4 It has been documented that drug use evaluation studies (DUE) are useful tools in healthcare delivery systems as they provide information on drug use patterns, facilitate rational use of drugs and identify high cost drugs (e.g. Antibiotics) which are of economic interests.5 In a quick literature review, we found that many studies deal with drug utilization in adults all over the world, while very few studies provide information on drug use patterns in pediatrics, particularly, antibiotic use patterns.2-4,6-9 Evidence from these studies confirms that antibiotics were prescribed to children inappropriately and in great amount and this irrational use considered one of the most important challenging global public health issues. Pediatrics considered to be one of the more susceptible groups to infectious diseases due to their special environments such as day care and schools which facilitate the transmission of drug resistant bacteria.6 In addition, children, ethically do not often involved in clinical trials and consequently, information about drugs effect in children is often insufficient. Furthermore, children incompliance to drug therapy either due to inconvenient dosing or multiple drug prescriptions is another important issue.6,8 Such challenges therefore, call for close monitoring of antibiotic prescribing trends in children and interventions should target pediatric clinical practice in order to optimize antibiotic use.
In Jordan, antimicrobials account for the largest market share of the drug consumption (23% by Jordanian dinars, 15% by unit) and unfortunately, very few antibiotics utilization research could be found in Jordan which revealed different patterns and inappropriate antibiotic prescriptions and dispensing.10-13 From these perspectives, it is crucial to perform studies on the current utilization patterns of antibiotics in Jordan as data from these studies would be expected to provide useful information in a field where such data is missing. To our knowledge, the current situation of antibiotic use in the outpatient pediatric settings in the Royal Medical Services /Jordan Armed Forces (RMS/JAF) is not well documented. Therefore, we design our study using World Health Organization (WHO) prescribing indicators and target pediatric patients with an aim to evaluate antibiotic prescribing patterns and related costs in the outpatient pediatric emergency clinic in (QRACH). Results of our evaluation will provide proper counseling in the pediatric emergency department and enhance awareness of the issue of antibiotic resistance between military prescribers in the RMS. Furthermore, they will help in developing an intervention programs aimed to optimize the use of antibiotics and thus decreasing the emergence of antibiotic resistance in outpatient settings at RMS military hospitals and consequently reducing the overall cost.
Methods
This study was conducted in the emergency pharmacy that provides services for the emergency department (ED) in (QRACH) which is the first specialized military referral hospital for children in Jordan. It is located within the campus of King Hussein Medical Center (one of the largest military hospital in Jordan). QRACH contains (200) beds and consisted of (13) sections of various fields of pediatric medicine. It provides services for children referred from all regions of Jordan and from neighboring countries.
We retrospectively surveyed a sample of (4530) prescriptions received from the outpatient pediatric emergency (PE) clinic in the hospital over a period of five consecutive months (December 2012- April 2013). These prescriptions were obtained using the emergency pharmacy electronic database. Simple random sampling was performed by one observer to select thirty prescriptions daily out of (234) prescriptions received from that clinic over the study period. The inclusion criteria were: prescriptions written during the study period include oral and intramuscular antibiotics and patients up to 14 years of age. Patients above 14 years old were excluded due to internal procedures followed in this facility to transfer this age group to other clinics assuming them to be adults. Throughout the study we followed the methodology recommended by the WHO for investigating drug use in a health facility. The following WHO core prescribing indicators were selected to be measured: the average number of drugs prescribed per encounter, the average number of antibiotics prescribed per encounter and the percentage of encounters in which an antibiotic was prescribed which is calculated as follows: (number of patients encounters with an antibiotic prescribed / total number of encounters surveyed) x 100%. An additional indicator, the percentage share of each antibiotic was also measured to identify the frequency of each antibiotic that was prescribed which is calculated as follows: (number of patients encounters with an individual antibiotic / total number of encounters with an antibiotic prescription) x 100%. We also selected to measure the distribution of diagnostic categories (e.g. percentage of all antibiotic prescriptions for respiratory conditions) that accounted for all antibiotic prescribing and the distribution of antibiotic prescribing for (URTIs). The data collected was analyzed to carry out descriptive analysis using Microsoft excel 2003 spread sheets and the Statistical Package for Social Sciences Version 16.
This study was approved by the Human Research Ethics Committee at the Royal Medical Services (RMS), (Application no. 2/2013 dated 11/2/2013).
Results
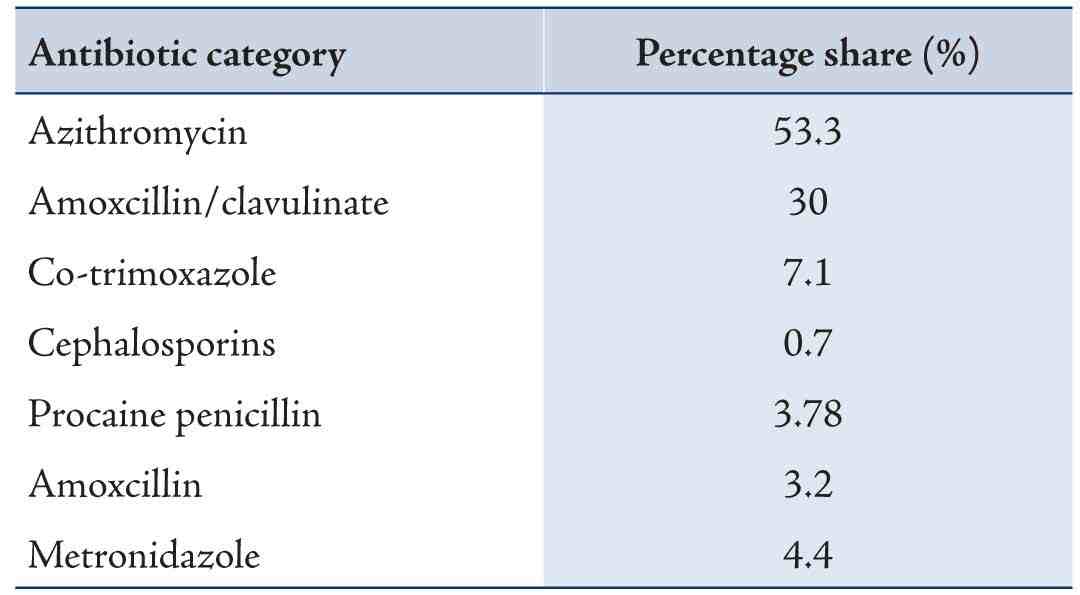
Out of the (4530) prescriptions received from the outpatient (PE) clinic over the study period, (3840) antibiotic prescriptions were counted out. The percentage of prescriptions involving antibiotics was (85%) as shown in Table 1. The average number of drugs per prescription was (2.4). Out of the surveyed antibiotic prescriptions (88%) contain one antibiotic, (11%) contain two antibiotics, and (1%) contain three antibiotics. The average cost of drugs on a prescription sheet was (1.259 JD), while the average cost of antibiotics was (0.668 JD). Table 2 shows the prescribing rate for each individual antibiotic category. Macrolides (most frequently azithromycin) and amoxicillin/clavulinate were the most commonly prescribed antibiotic groups with a percentage of (40%) and (25%) respectively. Azithromycin contributes to the highest percentage share of the macrolides category (97%). The most frequent diagnosis observed from the prescriptions was upper respiratory tract infections (URTIs) and accounted for (69%) of the diagnostic conditions in which antibiotic were prescribed as shown in (Table 3). Out of the (URTIs) prescriptions, we observed that common cold and acute bronchitis cases accounted for (32%), (25%) respectively, pneumonia cases (10%), tonsillitis (18%) and otitis media (15%). Azithromycin (53%) and amoxicillin/clavulinate (30%) account for the highest percentage share of prescribed antibiotics for URTIs (see Table 4).
Table 1: Indicators of Drug Use.
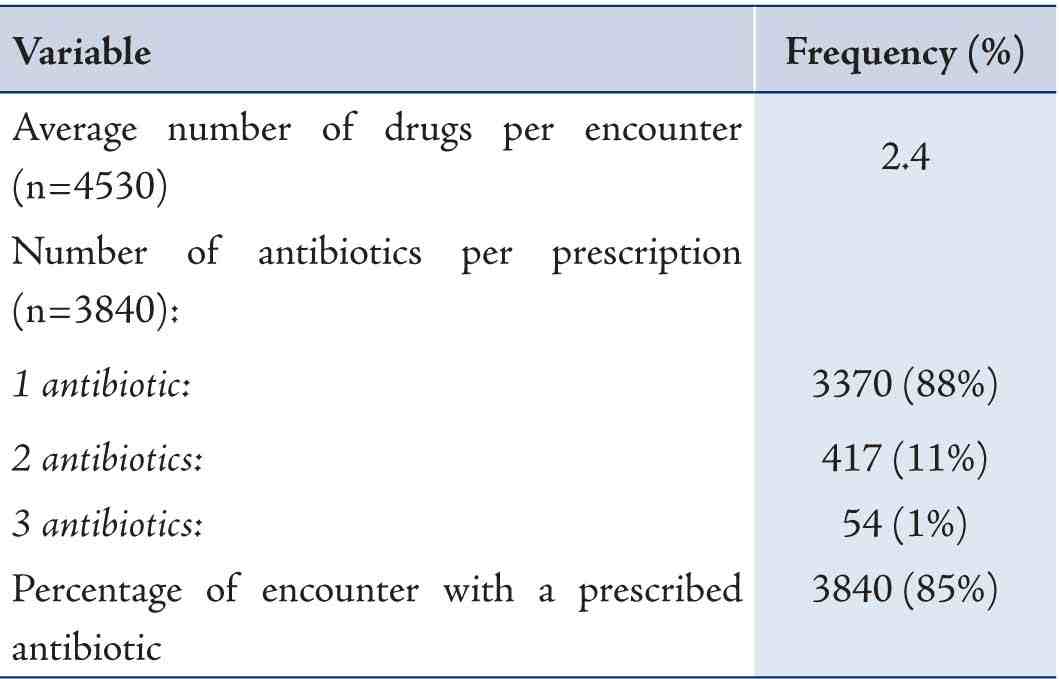
Table 2: Percentage Share of Prescribed Antibiotics.
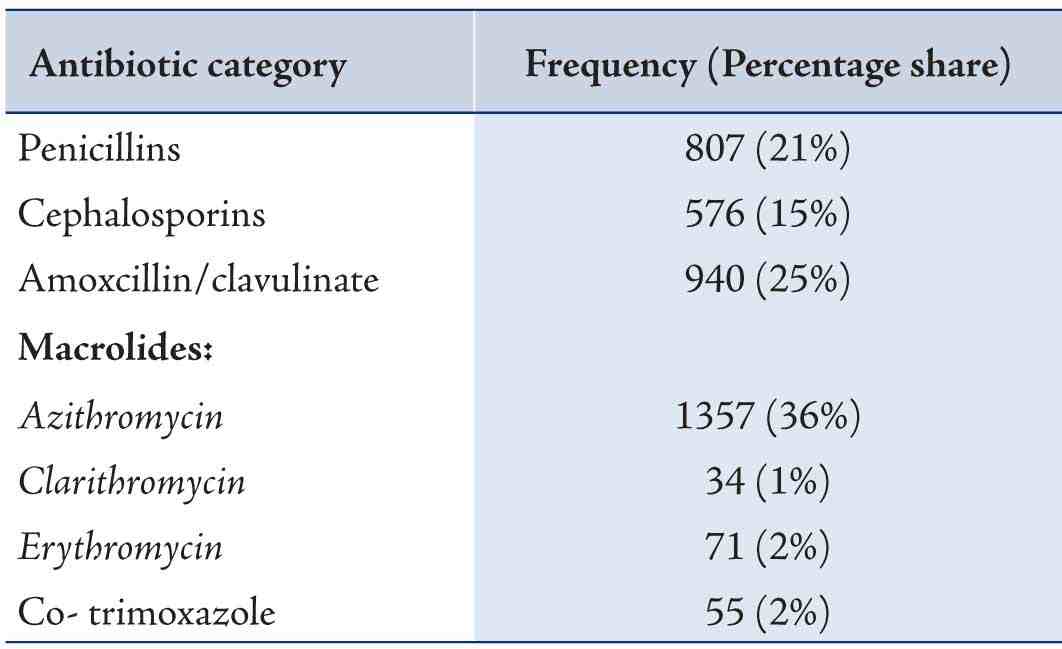
Table 3: Antibiotic Prescribing Patterns across Diagnostic. Conditions.

Table 4: Distribution of Antibiotic Prescribing for URTIs.
Discussion
It is documented that antibiotics in developing countries are consumed in relatively high levels and consequently led to higher occurrence of improper use and greater levels of resistance when compared to developed countries.14 Previous studies in developing countries shows that (35 to 60%) of clinical encounters were prescribed antibiotics while appropriate prescribing were reported in less than 20%.15 Hogerzeil et al., 1993,16 reported in their comparative analysis in twelve developing countries that (25 to 75) % of patients were prescribed antibiotics unnecessarily during clinical visits. Moreover, it has been reported that DUE studies of antibiotics in the outpatient environment is not as well established as in the inpatient settings.5 From these perspectives, we design such a study that would reflect, to a great extent, the current antibiotic- prescribing patterns in children in our setting. Accordingly, our data could provide some insights that may be applicable to other pediatric ambulatory care settings in both the community and other military hospitals and may guide future DUE studies in those settings.
This study reveals that antibiotic prescribing was frequent during pediatric visits to the ED resulting in a relatively high percentage of encounters. Our figure is higher than that reported in other pediatric outpatient settings as in Nigeria (41%),7 Kingdom of Saudi Arabia (19%),1 United States of America (21%)3 but almost similar to the value reported in India (81%) by Akhtar et.al, 2011.8
The high percentage rate of antibiotic prescribing in the outpatient (PE) clinic could point that emergency physicians are still holding the beliefs of the prophylactic role for antibiotics, especially when they feel pressured to prescribe antibiotics for those children with whom they stay with for short status and may be also sick to follow up with a pediatric consultant in a specialty clinic. In addition, absence of medical history of children attending the outpatient emergency clinic might influence the physicians’ decisions in prescribing antibiotics. Daily practice constraints and long working hours with the limited number of pediatric resident physicians in our setting could attribute also to the high prescription rate of antibiotics. Moreover, Conducting antibiotics audits, carrying out monitoring and supervision of physicians’ antibiotics prescribing practices are unfortunately absent in our setting. In a large survey in USA, Bauchner et. al, (1999)17 reported in their study that (50%) of the pediatricians prescribed antibiotics unnecessarily to children with viral infections during clinical visits after feeling pressure from their parents to do that. Several studies indicate that parental pressure to prescribe antibiotics and physician beliefs lead to increase rates of overprescribing.9,18 Parents attending the ED with their children might have different beliefs, different concerns and more satisfied to obtain an antibiotic prescription for their children than those attending traditional clinics. Although in our setting we did not investigate parents’ expectations and physician-parents communications and satisfactions regarding antibiotic prescribing; however, reports documented in other practice settings might be applicable and close to our setting and further studies will be required to investigate these aspects. The high rate of antibiotic percentage observed raises the need for auditing physicians in their prescribing practices of antibiotics, accordingly, reduction in the number of inappropriate prescriptions provided in the ED will be guaranteed.
Our results revealed that emergency pediatricians continue to prescribe broad spectrum antibiotics for outpatient children frequently, particularly for upper respiratory tract infections which were the most common medical condition observed in the surveyed prescriptions (see Table 3). Broad spectrum antibiotics accounted for approximately (60%) of the total prescribed antibiotics. (83%) of total antibiotics prescribed for URTIs were broad spectrum antibiotics; and macrolides (primarily azithromycin) were the leading class among them (see Table 2, Table 4) revealing that emergency pediatricians are prescribing broad spectrum antibiotics unnecessarily for common cold and acute bronchitis cases which are of virus etiology. In a recent study carried out in northern Jordan, children attending health centers with URTIs were prescribed antibiotics more often than adults (64% vs. 56%).11 Macrolides may constitute 2nd line agents in treatment guidelines in many of the reported cases in our facility and provide no clinical benefit, but promote the emergence of antibiotic-resistant organisms. Several previous studies have found large increases in the use of macrolides during the past decades due to their long half-life and short duration of therapy which make them an attractive antibiotic class and in some cases to target pathogens as Mycoplasma Pneumoniae as a cause of pneumonia.3 However, macrolides efficiency towards this pathogen has not been definitively established19 and resistance to this class has been reported among patients infected with community acquired pneumonia.20 Therefore, it would be wise for emergency physicians to avoid empirical macrolide therapy for children assuming the patient might be at risk of being infected with a macrolide resistant pathogen. In view of the above, future prospective studies are necessary to measure the degree of pediatricians’ adherence to clinical practices guidelines in our setting.
Our study showed that the average number of drugs per encounter is (2.4) which is slightly higher than the limit of (2.0) recommended by the WHO. However, the value falls at the midpoint of results reported by investigators from Kingdom of Saudi Arabia, Sudan, Nigeria, Yemen, Nepal ranging from (1.3 to 3.8)16 and close to that obtained by Otoom et.al, (2002)21 in Jordan (2.3). It has been reported that polypharmacy increases the risk of adverse drug reactions in children.7 Our finding reflects the fact that Jordan has reasonable practice towards polypharmacy in comparison with other developing countries.
The cost of medication is one of the key barriers for accessing medications in developing countries. It is documented that antibiotics are the most commonly prescribed class of drugs and have been reported to account for almost (50%) of the pharmacy budget in hospitals.8,22 In a study carried out in a primary healthcare in Spain, clinical inappropriateness was found to be (44%) of all cases given antibiotics, antibiotics not required but prescribed (28%) of all cases and costs of inappropriateness reached (68%) of the estimated total cost.23 Our study reveals that the cost of antibiotics is relatively high and accounts on average for almost half (53%) of the total cost of drugs on the prescription sheets. Our study, to some extent, is limited in cost implication of the prescribed antibiotics since we observed that (17%) of antibiotic prescriptions were written either with no diagnosis or with unclear diagnosis and since we cannot ensure the accuracy of the diagnosis for each visit included in the sampled prescriptions. Therefore, future prospective studies to measure the degree of appropriateness of antibiotic prescribing patterns and related cost in our setting and other military hospitals will be required.
It should be noted that we cannot ascertain the number of antibiotic prescriptions given to both patients who had an antibiotic and non-antibiotic responsive diagnosis because of the retrospective nature of our study. Therefore, we cannot assume that every antibiotic prescription included in our survey was unnecessary. Furthermore, the study was conducted in one outpatient setting and during the winter and spring seasons (December 2012- April 2013) which might influence the morbidity patterns and practices may have changed as a result of seasonal variations. However, these limitations do not detract from the study’s strength in documenting a high unacceptable rate of antibiotic prescriptions between military pediatricians in the ED and the study can be used as a quality project to monitor the use of antibiotics in the same setting.
Military prescribers and healthcare providers in the RMS/JAF should be aware of the problems associated with the over prescribing and over consumption of antibiotics particularly in pediatrics. Efforts should be targeted on emergency departments through establishing programs that reduce inappropriate antibiotic prescribing. This could be achieved through educational interventions that influence physicians performance in the form of Continuing Medical Education (CME) programs, CME sessions of small groups involving peers, delivery of a message by a local opinion leader, academic detailing (visits by trained physician educators such as pharmacists) and feedback system.5,24 Furthermore, Establishment of Drug and Therapeutic Committees (DTCs) that regularly review antibiotics utilization, conduct audits and carry out monitoring and supervision of military prescribers are warranted. Military prescribers should adopt the guidelines endorsed by the National Institute for Health and Clinical Excellence (NICE) which recommend either delaying or not prescribing antibiotic prescriptions for five common diagnosis; acute sore throat, acute otitis media, acute cough/bronchitis, acute sinusitis and common cold. This policy has approved to reduce antibiotic use for the above conditions up to (80%).25 Moreover, cost containment and cost reduction measures are necessary to optimize utilization of available resources without compromising the quality of care in view of limited resources and budget constraints particularly at the RMS and generally in Jordan. For example, establishing a higher fee system for expensive drugs such as antibiotics might be considered a cost-effective economic strategy to contain antibiotic over prescription. This was proven in a study that was carried out in Nepal which reported significantly lower percentage of antibiotic prescriptions and significantly higher percentage of prescriptions conforming to standard treatment GLs in health facilities charging a higher fee per expensive items such as antibiotics compared to those charging a flat fee per prescription.26 In addition, Parents need to recognize the value of antibiotics, the importance of using them for their children as required and avoid from them when unnecessary. Such behavioral changes can be done using educational programs and tools that are specially designed to target the parents such as using media i.e. radio and TV programs, distributing educational brochures and posters.
Conclusion
Antibiotic prescribing in the outpatient pediatric emergency clinic in our setting is relatively high and inappropriate to a great extent particularly broad spectrum antibiotics use in URTIs for which they are not indicated, on the contrary they have high cost and promote bacterial resistance. It must be stressed out that one of the most important tools for cost reduction is cost awareness and cost consciousness among different healthcare providers in the RMS. Interventions to promote rational and judicious prescribing between military pediatricians are required. Finally, this study needs to be extended and repeated over time to maintain good quality health care in the RMS military hospitals and to address factors influencing overprescribing of antibiotics between military prescribers.
Acknowledgements
The authors reported no conflict of interest and no funding was received on thos work.
References
1. Mohajer KA, Al-Yami SM, Al-Jeraisy MI, Abolfotouh MA. Antibiotic prescribing in a pediatric emergency setting in central Saudi Arabia. Saudi Med J 2011 Feb;32(2):197-198.
2. Alumran A, Hurst C, Hou X. Antibiotics Overuse in Children with Upper Respiratory Tract Infections in Saudi Arabia: Risk Factors and Potential Interventions. Clinical Medicine and Diagnostics 2011;1:8-16 .
3. Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics 2011 Dec;128(6):1053-1061.
4. Nash DR, Harman J, Wald ER, Kelleher KJ. Antibiotic prescribing by primary care physicians for children with upper respiratory tract infections. Arch Pediatr Adolesc Med 2002 Nov;156(11):1114-1119.
5. Boucher M, Vaillancourt R, McCarthy A. Drug use evaluation of oral antibiotics prescribed in the ambulatory care settings in the Canadian armed forces. Can J Clin Pharmacol 2003;10(1):5-10.
6. Nyquist AC, Gonzales R, Steiner JF, Sande MA. Antibiotic prescribing for children with colds, upper respiratory tract infections, and bronchitis. JAMA 1998 Mar;279(11):875-877.
7. Oshikoya K, Chukwura H, Ojo O. Evaluation of Outpatient Pediatric Drug Prescriptions in a Teaching Hospital in Nigeria for Rational Prescribing. Paediatr Perinat Drug Ther 2006;7:183-188 .
8. Akhtar MS., Vohora D., Pillai KK., Dubey K., Roy MS., Najmi A., Khanam R. Drug Prescribing Practices in Pediatric Department of a North Indian University Teaching Hospital. Asian Journal of Pharmaceutical and Clinical Research 2011;5:146-149.
9. Papaevangelou V, Rousounides A, Hadjipanagis A, Katsioulis A, Theodoridou M, Hadjichristodoulou C. Decrease of antibiotic consumption in children with upper respiratory tract infections after implementation of an intervention program in Cyprus. Antimicrob Agents Chemother 2012 Mar;56(3):1658-1661.
10. Mawajdeh S, Harvy K, Bader R. 2004. Jordanian Rational Use of Drugs Strategy Development Workshop; 2004 Sep 21-22; Dead Sea Valley/ Jordan. Available From: www. Docstoc. Com. [Cited 2013 May 15].
11. Al- Omari M, Yahia G, Khader Y, Batieha A, Dauod AS. Antibiotics in Upper Respiratory Tract Infections: Appropriateness of the Practice in Jordan. Jpn Med J 2010;44:413-419.
12. Sawair FA, Baqain ZH, Abu Karaky A, Abu Eid R. Assessment of self-medication of antibiotics in a Jordanian population. Med Princ Pract 2009;18(1):21-25.
13. Al-Azzam SI, Al-Husein BA, Alzoubi F, Masadeh MM, Al-Horani MA. Self-medication with antibiotics in Jordanian population. Int J Occup Med Environ Health 2007;20(4):373-380.
14. World Health Organization. 1996. The World Health Report. Geneva.
15. World Health Organization. 2001. Interventions and Strategies to Improve the Use of Antimicrobials in Developing Countries: Drug Management Program. Geneva: WHO; (WHO/CDS/CSR/DSR/2001.9).
16. Hogerzeil HV, Bimo, Ross-Degnan D, Laing RO, Ofori-Adjei D, Santoso B, et al. Field tests for rational drug use in twelve developing countries. Lancet 1993 Dec;342(8884):1408-1410.
17. Bauchner H, Pelton SI, Klein JO. Parents, physicians, and antibiotic use. Pediatrics 1999 Feb;103(2):395-401.
18. Kutty N. Treating children without antibiotics in primary healthcare. Oman Med J 2011 Sep;26(5):303-305.
19. Mulholland S, Gavranich JB, Chang AB. Antibiotics for community-acquired lower respiratory tract infections secondary to Mycoplasma pneumoniae in children. Cochrane Database Syst Rev 2010;(7):CD004875.
20. Daneman N, McGeer A, Green K, Low DE; Toronto Invasive Bacterial Diseases Network. Macrolide resistance in bacteremic pneumococcal disease: implications for patient management. Clin Infect Dis 2006 Aug;43(4):432-438.
21. Otoom S, Batieha A, Hadidi H, Hasan M, Al-Saudi K. Evaluation of drug use in Jordan using WHO prescribing indicators. East Mediterr Health J 2002 Jul-Sep;8(4-5):537-543.
22. Hasan M, Das M, Murad F. Drug Utilization and Antibiotic Use in the Primary Health Care Centers in Sharjah. East Mediterr Health J 1997;3:444-451.
23. File TM Jr. Solutions to the problem of bacterial resistance. Treat Respir Med 2005;4(Suppl 1):25-30.
24. Akande T, Ologe M, Medubi G. Antibiotic Prescription Pattern and Cost at University of Ilorin Teaching Hospital, Ilorin, Nigeria. International Journal of Tropical Medicine 2009;4:50-54.
25. National institute for health and clinical excellence. Prescribing of antibiotics for self-limiting respiratory tract infections in adults and children in primary care. Clinical guidance CG 69, July 2008. Accessed date 25th March. 2014.
26. Holloway KA, Gautam BR, Reeves BC. The effects of different kinds of user fees on prescribing quality in rural Nepal. J Clin Epidemiol 2001 Oct;54(10):1065-1071.
|