|
Abstract
Objectives: To determine the prevalence and incidence rates of Alzheimer’s disease (AD) between 1999 and 2010 in Wales and the relationship between AD with age.
Methods: The Patient Episode Database for Wales was used to identify patients who were diagnosed with AD between 1999 and 2010.
Results: During the 12-year study period, 14,534 people were diagnosed with AD in Wales. The overall prevalence of AD in individuals 60 years or older was 2% and the overall incidence was estimated as 1.5 per 1000 person-years. The prevalence of AD in individuals between 60 and 74 years was 1%, rising up to 5% in those aged 75 years and older. The incidence of AD increased during the study period from 1.4 per 1000 person-years in 1999 to 1.9 per 1000 person-years in 2010. More than half of the diagnosed AD during the study period was unspecified.
Conclusion: The incidence of Alzheimer’s disease is progressively increasing in Wales. Prevalence and incidence rates rise with age. It is important that the public is educated on the symptoms of AD and doctors pay particular attention to these symptoms so as to ensure that diagnosis is made as early as possible. This will enable adequate support to be provided as soon as possible in order to prolong patients’ independence and slow the progression of symptoms.
Keywords: Dementia; Alzheimer’s disease; Wales; early-onset Alzheimer’s disease; late-onset Alzheimer’s disease; incidence; prevalence; Unspecified; epidemiology; United Kingdom.
Introduction
There is a rapidly progressive increase in ageing population around the world, especially in developed countries such as the United Kingdom, Japan and Germany. The World Health Organization has estimated that by 2025, the population of people aged 60 and over will be approximately 1.2 billion, increasing by 223% from the population in 1970.1 In the United Kingdom, Wales was consistently the most aged between 1985 and 2010 among the four UK constituent countries, with the highest proportion of people aged 65 and over in its population.2 Approximately one-fifth of the population of Wales are aged 65 years and over.2 With an increasing ageing population comes medical problems such as dementia.
Dementia is a common problem among the growing elderly population in developed countries such as the United Kingdom. In 2009, it was estimated that 35.6 million people will be living with dementia in 2010 and will almost double every 20 years to 65.7 million in 2030 and 115.4 million in 2050 worldwide.3 In the United Kingdom, it is estimated that 821,884 people have dementia,4 with an additional more than 400,000 remaining undiagnosed.5
Dementia is the third leading cause of death in the United States of America, on a par with cerebrovascular diseases.6 Dementia can be extremely debilitating affecting cognitive areas such as attention, memory, problem solving and language. Early signs of Alzheimer’s disease (AD) include unusual memory loss and logopenic progressive aphasia. As the disease progresses, individuals begin to have mood swings and have difficulty performing complex activities such as driving. In the later stage of the disease, they forget how to do simple activities such as brushing their teeth, and ultimately end up requiring full-time care.
Alzheimer’s disease (AD) is the commonest cause of dementia accounting for more than 60% of cases.7 There have been several studies on the incidence of dementia, however many have been based on single site or only within a suburb of cities.8,9 Studies on the incidence of Alzheimer’s disease are even more limited. In the United States of America, it has been suggested that the prevalence of AD is 10% among individuals aged 71 and older10 while it has been estimated that the prevalence is 4% in Europe in individuals 65 years and older.11
There are three main types of AD – early-onset AD (before age 65 years), late-onset AD (after age 65 years) and familial AD. Early-onset AD is a rare form of AD, with symptoms developing before the age of 65 years. It accounts for only 6-7% of all cases of Alzheimer’s disease.12,13 Early-onset AD could be familial or sporadic, but most patients with early-onset AD do not have a familial disorder.14 Individuals with early-onset familial AD would usually have at least one first-degree relative with a history of AD. Late-onset AD is the commonest type of AD accounting for approximately 95% of all cases of Alzheimer’s disease.15 Several genetic studies have shown that individuals with an APOEå4 genetic variant are at an increased risk of late-onset AD.16,17 Familial AD is an extremely rare form of AD with an estimated 600 affected individuals in England and Wales.18 It is usually inherited in an autosomal dominant pattern. There are three main gene mutations that have been implicated in familial Alzheimer’s disease - Amyloid beta (A4) precursor protein (APP),19 Presenilin 1 (PSEN1)20 and Presenilin 2 (PSEN2).21
There is no recent study in the literature on the epidemiology of AD among the elderly in Wales. As the ageing population is increasing in Wales, it would be expected that the incidence of AD would have increased over the study period and therefore important to understand the current trends of AD in the country. The knowledge of the distribution and occurrence of AD could facilitate a further understanding of its pathology and would also highlight public health issues that need to be addressed in Wales. In Wales, the Patient Episode Database for Wales (PEDW) contains all inpatient and day case activity undertaken in National Health Service (NHS) Wales in addition to data on Welsh residents treated in English Trusts. The aims of this study were to determine the prevalence and incidence rates of AD between 1999 and 2010 in Wales and the relationship between AD with age.
Methods
AD was diagnosed using the International Statistical Classification of Diseases and Related Health Problems [Version 10] (ICD-10) diagnosis codes:
G300 – Alzheimer’s disease with early onset
G301 – Alzheimer’s disease with late onset
G308 – Other specified Alzheimer’s disease
G309 – Unspecified Alzheimer’s disease
The diagnosis of AD relied solely on the diagnosis codes entered into PEDW.
The Patient Episode Database for Wales (PEDW) was implemented in April 1991. It contains all inpatient and day case activity undertaken in NHS Wales in addition to data on Welsh residents treated in English Trusts. The population of Wales is predominantly of white European ethnicity with ethnic minorities comprising just 3% of the population. The demographics of the region has remained stable for a number of decades with annual inward and outward migration rates of <1% of the population. Individual records are submitted to PEDW on the basis of a patient’s consultant episode, which is the time an admitted patient spends in the continuous care of one consultant within one NHS trust. Information recorded includes age and sex of patients, month and year of admission, and diagnosis. Data were collected on AD diagnosis that was recorded in PEDW in the fiscal year in which they were reported. All patients diagnosed with AD between 1999 and 2010 were included in this study, with particular emphasis on patients aged 60 years and above.
The incidence of AD was calculated using the mid-year population estimates of Wales for each year of the study.22 The rates were expressed per 1000 person-years. A Poisson regression model was fitted to assess temporal trends.23 Rate ratios (RR) and 95% confidence intervals (CI) were determined and compared over the study period. The data were analysed using SPSS version 18.0 and the level of statistical significance at which the null hypothesis was rejected was chosen as 0.05.
Results
There were a total of 14,534 people diagnosed with Alzheimer’s disease between 1999 and 2010 (Table 1). More than 97% of these people were older than 60 years. This is equivalent to approximately 1211 cases annually in Wales and 1178 cases yearly among patients who are 60 years and older. The annual incidence of AD among the elderly was estimated to 1.5 per 1000 person-years or 153.5 per 100,000 in the general elderly population. The prevalence of AD among individuals between 60-74 years is 1% and 5% among individuals 75 years and older. In the initial period of the study, the overall incidence of AD among people who are 60 years and older remained relatively constant (1.4 per 1000 person-years). However, since 2004, the incidence has increased ranging from 1.5-1.9 per 1000 person-years annually (Table 2).
Table 1: Number of people diagnosed with Alzheimer’s disease in the Patient Episode Database for Wales 1999-2010 fiscal year.
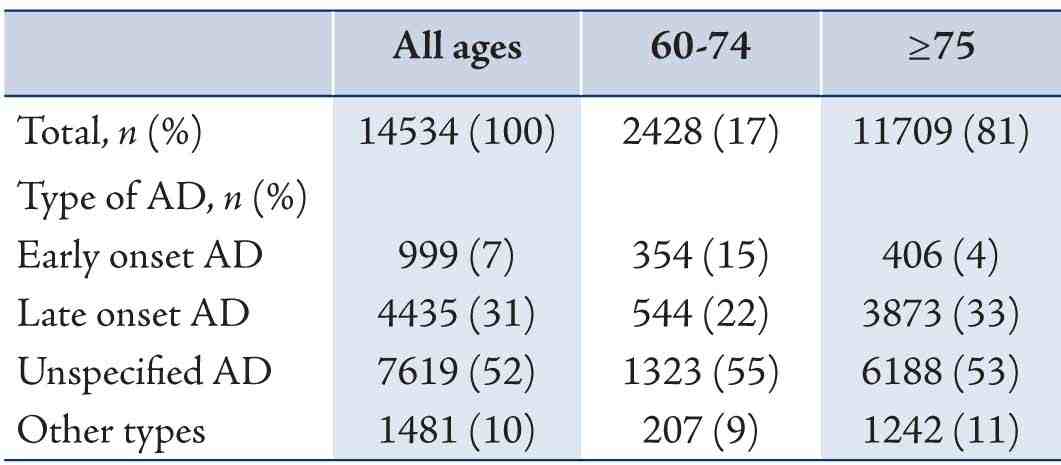
Table 2: Incidence rates of Alzheimer’s disease in individuals 60 years and older in Wales.
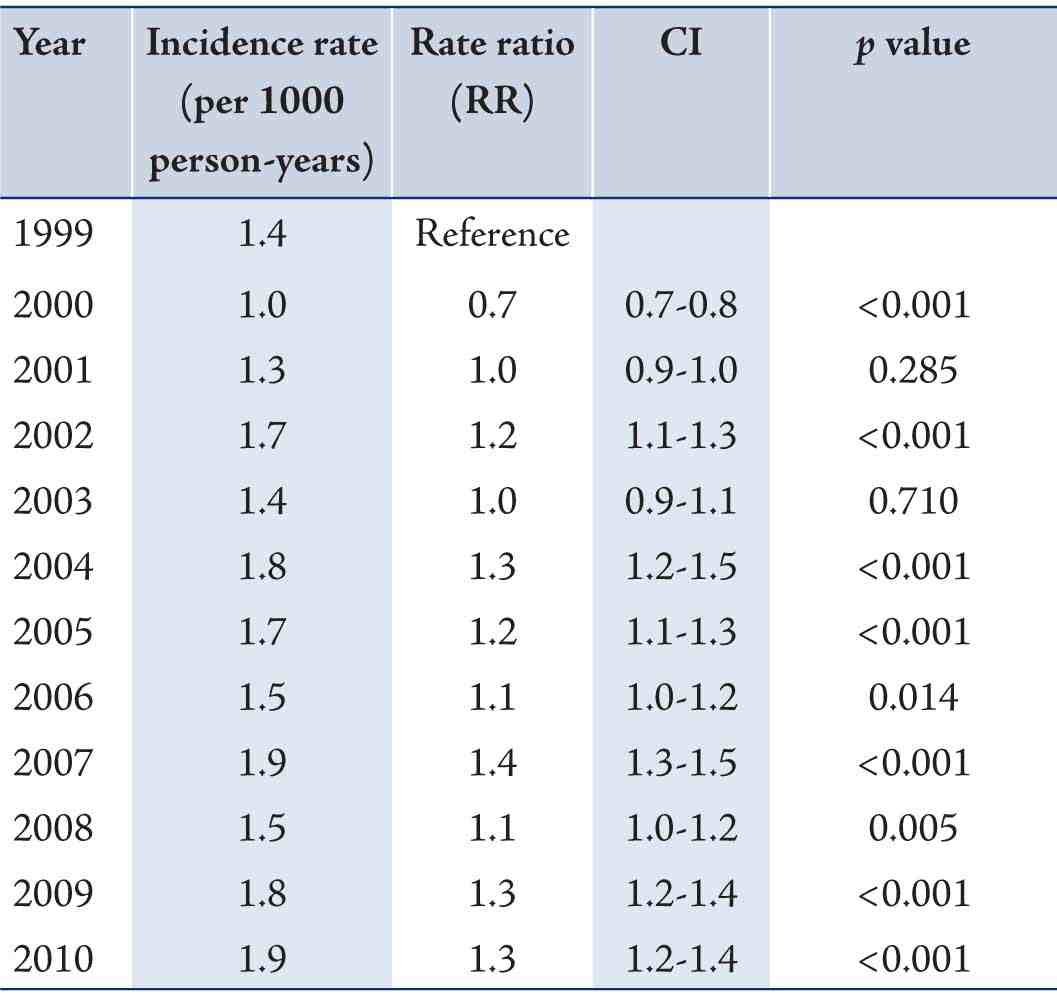
CI: Confidence Interval
There were more people with AD in the ≥75 age group than the 60-74 age group (RR 4.8 [CI 4.6-5.0], p<0.001). The incidence rate among the ≥75 age group was estimated to 3.7 per 1000 person-years while in the 60-74 age group, it was 0.4 per 1000 person-years. The incidence has remained relatively stable in the 60-74 age group, but has been increasing progressively in patients who are 75 years and older during the study period (Fig. 1). More than half of the diagnosed AD during the study period was unspecified (RR 9.9 [CI 9.2-10.6], p<0.001). Late-onset AD and ‘Other specified’ AD are significantly more common than early-onset AD [(RR 5.8, p<0.001) and (RR 1.9, p<0·001) respectively]. Early-onset AD accounted for 7% of all cases of AD diagnosed during the study period (Table 1). There has been more than a 40-fold increase in the number of individuals diagnosed with ‘Other specified’ AD between 1999 and 2010. The number of individuals with early-onset AD in the 60-74 age group remained relatively constant in the first 5 years of the study with an average of 16 patients annually, but more than doubled in 2004 (Fig. 2). The number of early-onset AD diagnosed in this age group remained that high through to 2010 with an average of 39 cases annually. However, the number of late-onset Alzheimer’s disease in the 60-74 age group continues to drop in the later part of study period (Fig. 2).
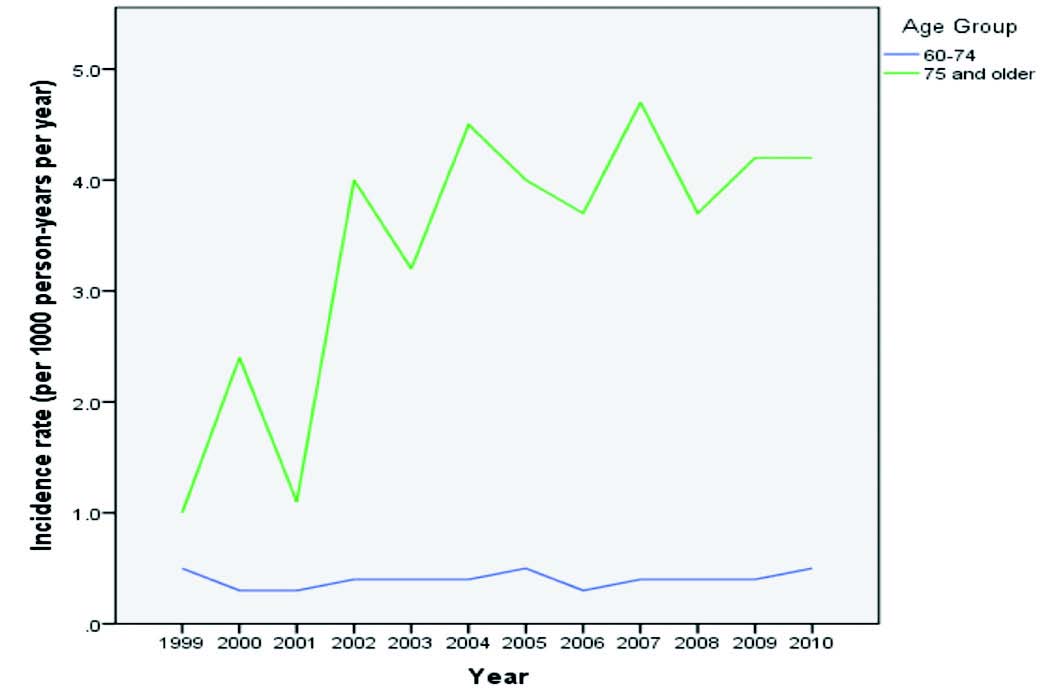
Figure 1: Overall annual incidence of Alzheimer’s disease. Incidence has remained relatively stable in the 60-74 age group, but has been increasing progressively in patients who are 75 years and older between 1999-2010.
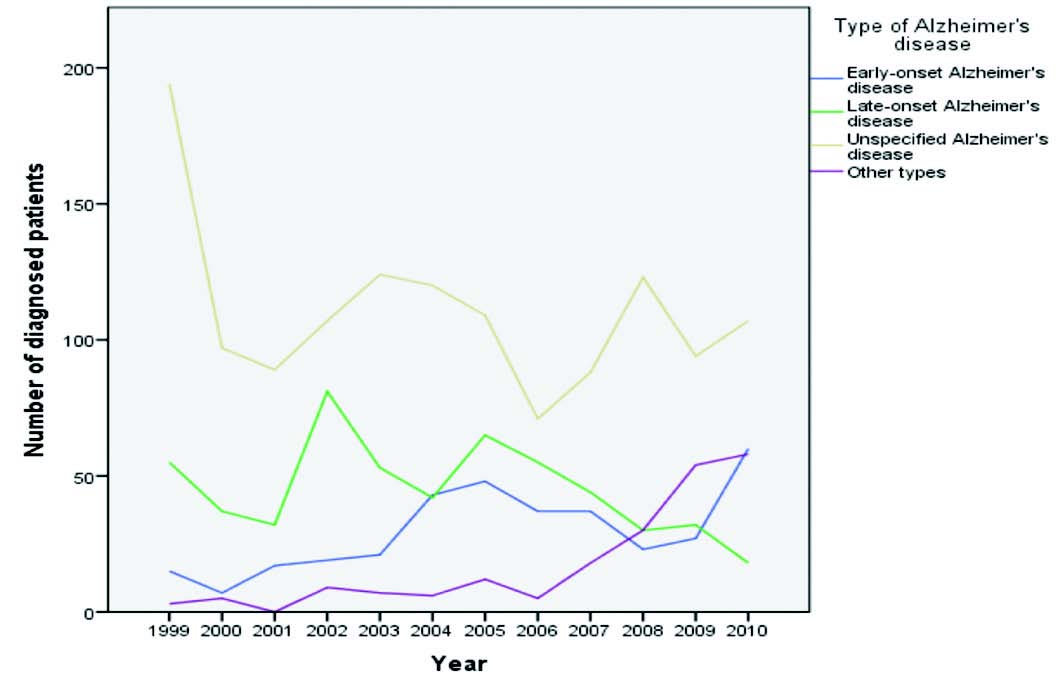
Figure 2: Trends of the types of Alzheimer’s disease in the 60-74 age group between 1999 and 2010.
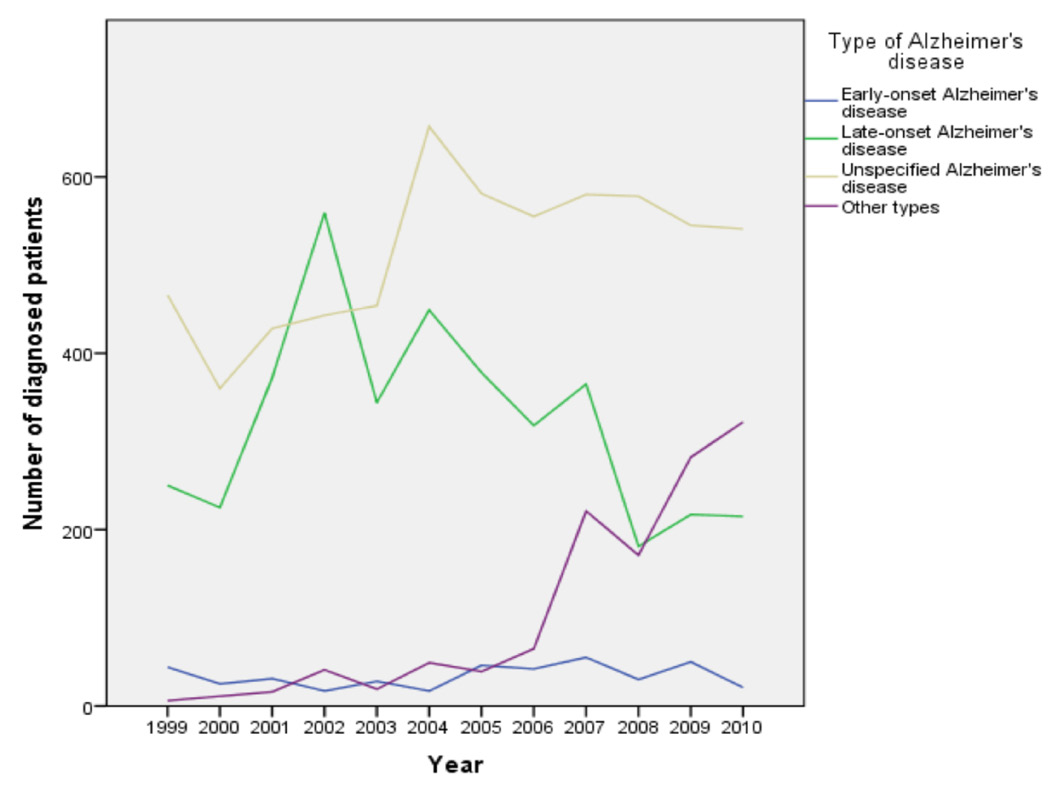
Figure 3: Trends of the types of Alzheimer’s disease in individuals 75 years and older between 1999 and 2010.
Among individuals 75 years and older, most of the AD diagnosis were unspecified and the number of individuals in this category remained high during the study period (Fig. 3). However, the incidence of late-onset AD appears to be dropping in the later part of the study period (Fig. 3). The number of AD diagnosis classified as ‘Other types’ continues to rise during the study period (Fig. 3). Early-onset AD also accounts for approximately 4% of AD diagnosed in the ≥75 age group during the study period (Table 1).
Discussion
This is one of the largest studies on the epidemiology of Alzheimer’s disease in Europe. It is also the first study on the trends of Alzheimer’s disease in Wales. Contrary to previous studies that were based on hospital or single city cohorts, this study is based on data from a public register that includes cases from the whole country. This study has been facilitated by the availability of a single robust registry in Wales that has systematically collected records over more than a decade. The ethnic homogeneity and relative stability of our population limit confounding influences from ethnicity and migration that may be difficult to control in larger heterogeneous populations.
This study has demonstrated that AD is a significant problem among persons older than 60 years. There were a total of 14,534 people diagnosed with AD between 1999 and 2010, more than 97% of whom were 60 years or older. The overall prevalence of AD in individuals 60 years or older was 2% and the overall incidence was estimated to 1.5 per 1000 person-years. However, this is likely to be significantly underestimated as only patients who present to doctors are included in the Welsh database. It is therefore very much likely that many people with AD remain undiagnosed in the community. The overall prevalence in this study is significantly lower than in the United States of America where as high as 10% of those over the age of 65 years are estimated to have Alzheimer’s disease.24 Alzheimer’s disease is known to be associated with poverty and illiteracy.25 It is very much possible that the significantly higher prevalence of Alzheimer’s disease in America is partly related to these factors where such factors are more prevalent than Wales.
Prevalence increases steeply with age, from 1% among the 60-74 age group to approximately 5% among individuals 75 years and older. This trend is similar to previous studies in the literature.9,26 The incidence rate also appears to increase with age. In the 60-74 age group, it was estimated to 0.4 per 1000 person-years while in the ≥75 age group, it is approximately 4.0 per 1000 person-years. While this trend in incidence rate is similar to other studies, the actual incidence rate of Alzheimer’s disease appears to be lower than in other countries. The overall annual incidence of AD among individuals older than 60 years is estimated to 1.5 per 1000 person-years. This is significantly lower than the estimated incidence in Japan,27 Italy28 and the United States of America.29
In the initial period of the study, the overall incidence of AD among people who were 60 years and older remained relatively constant (1.4 per 1000 person-years). However, since 2004, the incidence has increased ranging from 1.5-1.9 per 1000 person-years annually. This could either be due to improved diagnosis by physicians or an actual increase in incidence rate of AD. However, while the former may contribute to the increase in incidence rate, it is more likely that the increase is largely due to the latter because of the increasing ageing population in Wales.
More than half of the diagnosed AD during the study period was unspecified. Hence, it is unknown whether these were early-onset, late-onset or familial AD. As this is a significant number, it is likely that this could affect the analyses of the sub-types of AD. It is therefore recommended that physicians take more detailed history and record more comprehensive diagnosis, which will help to improve the quality of data in the registry. These could facilitate future study of precursors and natural history of Alzheimer’s disease.
Late-onset AD and ‘Other specified’ AD are significantly more common than early-onset AD. Early-onset AD accounts for 7% of all cases of AD diagnosed during the study period in Wales, which is comparable to previous reports.12,13 Early-onset Alzheimer’s disease is a rare form of AD that occurs in individuals before the age of 65 years. The fact that this type of AD was diagnosed in those older than 65 years in this study would suggest that the diagnosis was based on history of prolonged progressive dementia that probably began before the age of 65 years. This could imply that there is delay in the diagnosis of early-onset AD and that the diagnosis is being completely missed in a large number of people in Wales. It may also be an indication that there is equally delay in the diagnosis of late-onset AD, especially as it may first be associated with natural process of ageing. It is therefore recommended that the public is adequately educated on the symptoms of AD in order to improve early presentation to doctors. This will enable adequate support to be provided to prolong patients’ independence and slow the progression of symptoms. There was a progressive rise in ‘Other types’ AD in both the 60-74 and ≥75 age groups during the study period. This may suggest that we are beginning to see a rise in the prevalence and incidence rates of familial Alzheimer’s disease in Wales. However, more studies are needed to confirm this hypothesis. Although the incidence of late-onset AD appears to be dropping in both the 60-74 and ≥75 age groups, the continued high number of diagnosis classified as ‘Unspecified’ may be masking the actual incidence of late-onset AD. There is therefore need to improve on this aspect of diagnosis and documentation.
The study has limitations. As with all database research, the findings rely on the quality of the coded data. Some of the AD cases were classified as ‘Unspecified’; hence the actual prevalence and incidence rates of early-onset and late-onset AD among old people in Wales may be significantly higher. Expansion of the currently held datasets for Alzheimer’s disease in the Welsh database to incorporate more comprehensive diagnosis details will allow better insights into current trends of Alzheimer’s disease. In addition, only patients who present to doctors are included in the Welsh database, therefore there are probably many more people in the community who remain undiagnosed.
Conclusion
Alzheimer’s disease is a major problem among the elderly in Wales. While it initially affects cognitive function, it ultimately affects people’s activities of daily living. Although this study has its limitations, it has provided some insights into the epidemiology of Alzheimer’s disease in Wales for the first time. The overall prevalence of AD in individuals 60 years or older is 2% and the overall incidence is estimated to 1.5 per 1000 person-years in Wales. However, this is likely to be significantly underestimated as only patients who present to doctors are included in the Welsh database. It is therefore very much likely that many people with AD remain undiagnosed in the community. Nevertheless, the incidence of AD is progressively increasing in Wales. Prevalence and incidence rates increase with age. It is important that the public is educated on the symptoms of AD and doctors pay particular attention to these symptoms so as to ensure that diagnosis is made as early as possible. This will enable adequate support to be provided as soon as possible in order to prolong patients’ independence and slow the progression of symptoms.
Acknowledgements
The authors reported no conflict of interest and no funding was received on this work.
References
1. World Health Organisation. Active ageing: a policy framework [Internet]. Geneva: World Health Organisation; 2002 [cited 15th June 2014]. Available at: http://whqlibdoc.who.int/hq/2002/WHO_NMH_NPH_02.8.pdf
2. Office for National Statistics. Population ageing in the UK, its constituent countries and the European Union [Internet]. Newport: Office for National Statistics; 2012 [cited 15th June 2014]. Available at: http://www.ons.gov.uk/ons/dcp171776_258607.pdf
3. Alzheimer’s Disease International. World Alzheimer Report 2009: The benefits of early diagnosis and intervention. London: Alzheimer’s Disease International; 2009
4. University of Oxford Health Economics Research Centre. Dementia 2010: The economic burden of dementia and associated funding in the United Kingdom. Cambridge: Alzheimer’s Research Trust; 2010
5. Alzheimer’s society. Increase in number of people diagnosed with dementia: over 400,000 remain undiagnosed, according to Alzheimer’s Society [Internet]. London: Alzheimer’s Society; 2012 [cited 15th June 2014]. Available at: https://www.alzheimers.org.uk/site/scripts/news_article.php?newsID=1164
6. Ewbank DC. Deaths attributable to Alzheimer’s disease in the United States. Am J Public Health 1999 Jan;89(1):90-92.
7. Alzheimer’s society. Demography. London: Alzheimer’s Society [Updated July 2013; cited 15th June 2014]. Available at: http://alzheimers.org.uk/site/scripts/documents_info.php?documentID=412
8. Ott A, Breteler MM, van Harskamp F, Stijnen T, Hofman A. Incidence and risk of dementia. The Rotterdam Study. Am J Epidemiol 1998 Mar;147(6):574-580.
9. Hebert LE, Scherr PA, Beckett LA, Albert MS, Pilgrim DM, Chown MJ, et al. Age-specific incidence of Alzheimer’s disease in a community population. JAMA 1995 May;273(17):1354-1359.
10. Plassman BL, Langa KM, Fisher GG, Heeringa SG, Weir DR, Ofstedal MB, et al. Prevalence of dementia in the United States: the aging, demographics, and memory study. Neuroepidemiology 2007;29(1-2):125-132.
11. Lobo A, Launer LJ, Fratiglioni L, Andersen K, Di Carlo A, Breteler MM, et al; Neurologic Diseases in the Elderly Research Group. Prevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurology 2000;54(11)(Suppl 5):S4-S9.
12. Campion D, Dumanchin C, Hannequin D, Dubois B, Belliard S, Puel M, et al. Early-onset autosomal dominant Alzheimer disease: prevalence, genetic heterogeneity, and mutation spectrum. Am J Hum Genet 1999 Sep;65(3):664-670.
13. Nussbaum RL, Ellis CE. Alzheimer’s disease and Parkinson’s disease. N Engl J Med 2003 Apr;348(14):1356-1364.
14. Joshi A, Ringman JM, Lee AS, Juarez KO, Mendez MF. Comparison of clinical characteristics between familial and non-familial early onset Alzheimer’s disease. J Neurol 2012 Oct;259(10):2182-2188. Epub ahead of print.
15. Gaj P, Paziewska A, Bik W, Dąbrowska M, Baranowska-Bik A, Styczynska M, et al. Identification of a late onset Alzheimer’s disease candidate risk variant at 9q21.33 in Polish patients. J Alzheimers Dis 2012;32(1):157-168. Epub ahead of print.
16. Corder EH, Saunders AM, Strittmatter WJ, Schmechel DE, Gaskell PC, Small GW, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 1993 Aug;261(5123):921-923.
17. Strittmatter WJ, Saunders AM, Schmechel D, Pericak-Vance M, Enghild J, Salvesen GS, et al. Apolipoprotein E: high-avidity binding to beta-amyloid and increased frequency of type 4 allele in late-onset familial Alzheimer disease. Proc Natl Acad Sci U S A 1993 Mar;90(5):1977-1981.
18. Liddell MB, Lovestone S, Owen MJ. Genetic risk of Alzheimer’s disease: advising relatives. Br J Psychiatry 2001 Jan;178(1):7-11.
19. Goate A, Chartier-Harlin MC, Mullan M, Brown J, Crawford F, Fidani L, et al. Segregation of a missense mutation in the amyloid precursor protein gene with familial Alzheimer’s disease. Nature 1991 Feb;349(6311):704-706.
20. Sherrington R, Rogaev EI, Liang Y, Rogaeva EA, Levesque G, Ikeda M, et al. Cloning of a gene bearing missense mutations in early-onset familial Alzheimer’s disease. Nature 1995 Jun;375(6534):754-760.
21. Levy-Lahad E, Wasco W, Poorkaj P, Romano DM, Oshima J, Pettingell WH, et al. Candidate gene for the chromosome 1 familial Alzheimer’s disease locus. Science 1995 Aug;269(5226):973-977.
22. StatsWales. Population of Wales. Statistics Wales 1999-2010 [Internet]. Cardiff: Welsh Government [cited: 27th July 2012] http://www. http://statswales.wales.gov.uk/
23. Frome EL, Checkoway H. Epidemiologic programs for computers and calculators. Use of Poisson regression models in estimating incidence rates and ratios. Am J Epidemiol 1985 Feb;121(2):309-323.
24. Evans DA, Funkenstein HH, Albert MS, Scherr PA, Cook NR, Chown MJ, et al. Prevalence of Alzheimer’s disease in a community population of older persons. Higher than previously reported. JAMA 1989 Nov;262(18):2551-2556.
25. Launer LJ, Andersen K, Dewey ME, Letenneur L, Ott A, Amaducci LA, et al. Rates and risk factors for dementia and Alzheimer’s disease: results from EURODEM pooled analyses. EURODEM Incidence Research Group and Work Groups. European Studies of Dementia. Neurology 1999 Jan;52(1):78-84.
26. Graves AB, Larson EB, Edland SD, Bowen JD, McCormick WC, McCurry SM, et al. Prevalence of dementia and its subtypes in the Japanese American population of King County, Washington state. The Kame Project. Am J Epidemiol 1996 Oct;144(8):760-771.
27. Lee JY, Chang SM, Jang HS, Chang JS, Suh GH, Jung HY, et al. Illiteracy and the incidence of Alzheimer’s disease in the Yonchon County survey, Korea. Int Psychogeriatr 2008 Oct;20(5):976-985.
28. Di Carlo A, Baldereschi M, Amaducci L, Lepore V, Bracco L, Maggi S, et al; ILSA Working Group. Incidence of dementia, Alzheimer’s disease, and vascular dementia in Italy. The ILSA Study. J Am Geriatr Soc 2002 Jan;50(1):41-48.
29. Bachman DL, Wolf PA, Linn RT, Knoefel JE, Cobb JL, Belanger AJ, et al. Incidence of dementia and probable Alzheimer’s disease in a general population: the Framingham Study. Neurology 1993 Mar;43(3 Pt 1):515-519.
|