|
Introduction
Trauma in children has been a concern but given little attention. Lately however, in Oman, it has been widely discussed in light of prevention of road traffic accidents and home accidents. Trauma in children comes only second to acute infection responsible for morbidity in children, with an annual cost of over £200 millions per year in UK.1 However, there are no cost figures from gulf countries currently available.
In Oman, all limb fractures are managed in the regional referral hospitals established in all regions of the country. A good network of referral system exists for referring and transport of children from local health centers to regional referral hospitals, which are staffed by well trained specialized trauma units. There is a steady increase in hospital admission rates from accidental injuries, but there are no published data on the pattern, management and outcome of limb fractures in the pediatric age group.
Keeping in mind the above mentioned facts, an audit of pediatric limb fracture at Nizwa regional referral hospital, was conducted to evaluate; a) the annual inpatient workload arising from pediatric limb fractures, b) pattern of fractures and their management, and c) areas where management could be improved.
Pediatric trauma has low priority and as such has been given little attention. The aim of this study is to review and audit the pattern of pediatric fractures, their management and outcome in our local setting.
Methods
This is a retrospective review of 270 children aged up to 12 years with limb fractures admitted to the pediatric orthopedic ward of Nizwa hospital, between January 2007 to December 2008.
The exclusion criteria included; children with pathological fractures of limbs, skull, spine, and pelvis and rib fractures, severe injuries admitted under general surgery, and those who were transferred to tertiary centres.
Data was recorded in a computer database and it contained date of admission, discharge, progress, operation notes and follow up visits. The data was checked for completeness and accuracy by cross- referencing against nursing, operation records along with patient progress notes and radiographs. All patient data was assessed in terms of the following parameters; age, sex, date of admission, diagnosis (ICD Code), treatment, mechanism of injury, operation data and date of discharge. Age specific admission rates were performed using 2001 population census data for the Al Dakhliya region.
Management was audited by studying the treatment methods employed (conservative/operative), duration of hospital stay, unplanned readmission and radiographic outcomes, plus the need for any secondary operative intervention or salvage internal fixation, complications and any associated injuries.
Results
Al Dakhliya region in 2007-2008 had an estimated pediatric population (0-12 years) of approximately 27% of the total population of 2, 35,337. During this period, 270 children of whom 202 (74.8%) were boys and 68 (25.2%) girls, were admitted to the pediatric orthopedic ward with limb fractures. This was estimated to be around 42/10000 of the local pediatric population. The patient age ranged between 1+/-12 years with a mean of 7.2+ /-2.1 years.
Of the studied patients, 210 (78%) were admitted through accident and emergency department, 56 (20.7%) were transferred from other peripheral hospitals and health centres, and 4 (1.6%) after being seen in fracture clinics.
The admission rates were reported to vary with the age and sex of the patients. The admission rate was observed most commonly in children of independent walking age and even more commonly in the early teens. These parameters were predominantly boys, (Fig. 1). In the 270 children admitted with limb fractures, the majority of the fractures were closed 266 (98.5%), while 4 (1.5%) patients had open fractures. The most common site of fracture was seen in forearm bones 100 (37%), followed by the shaft femur 48 (17.8%), lower end humerus 44 (16.2%), tibia 28 (10.3%), shaft humerus 13 (4.9%) and other fractures of the hand and foot bones accounted for 37 (13.7%) cases. (Fig. 2)
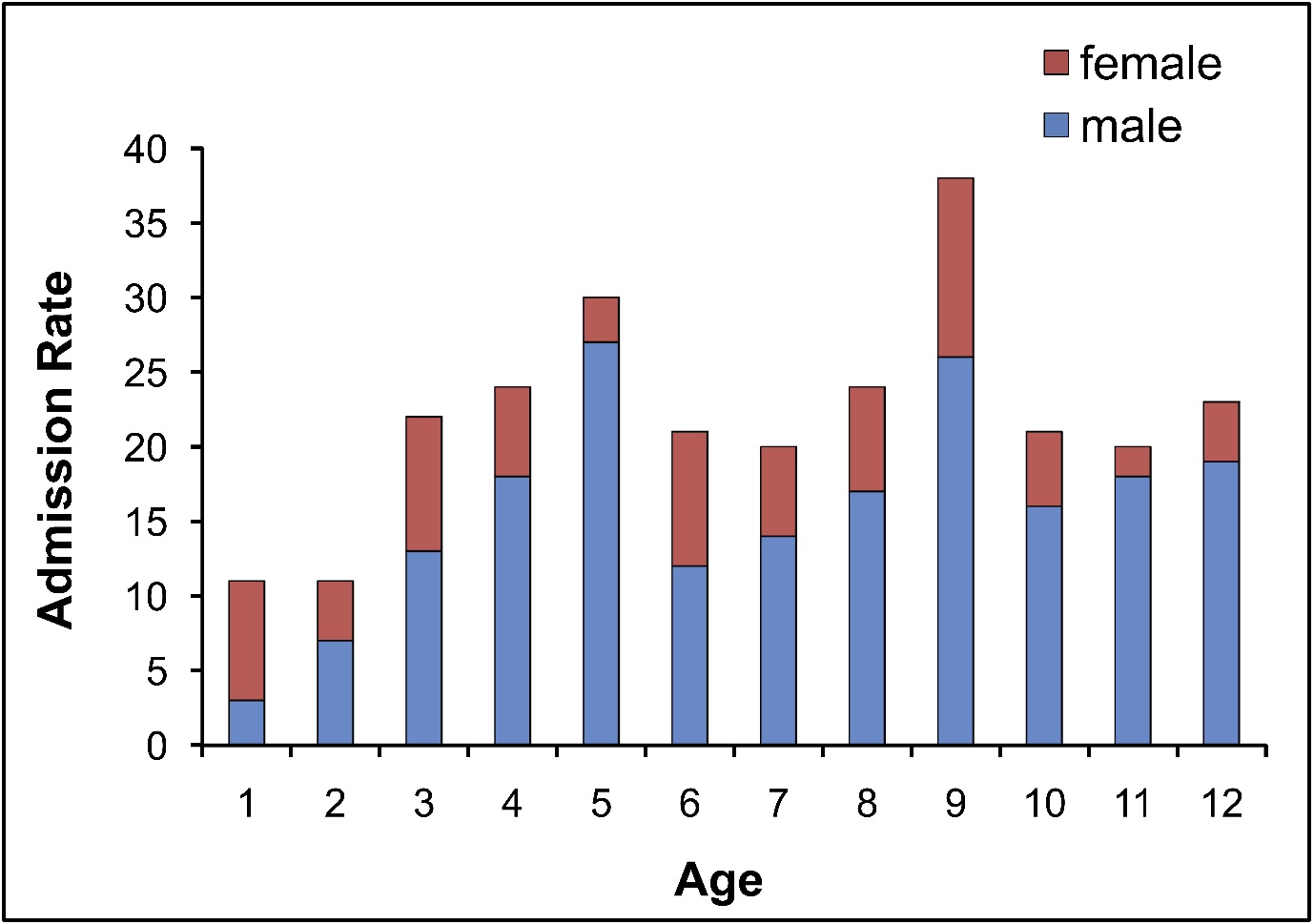
Figure 1: Admission rates.
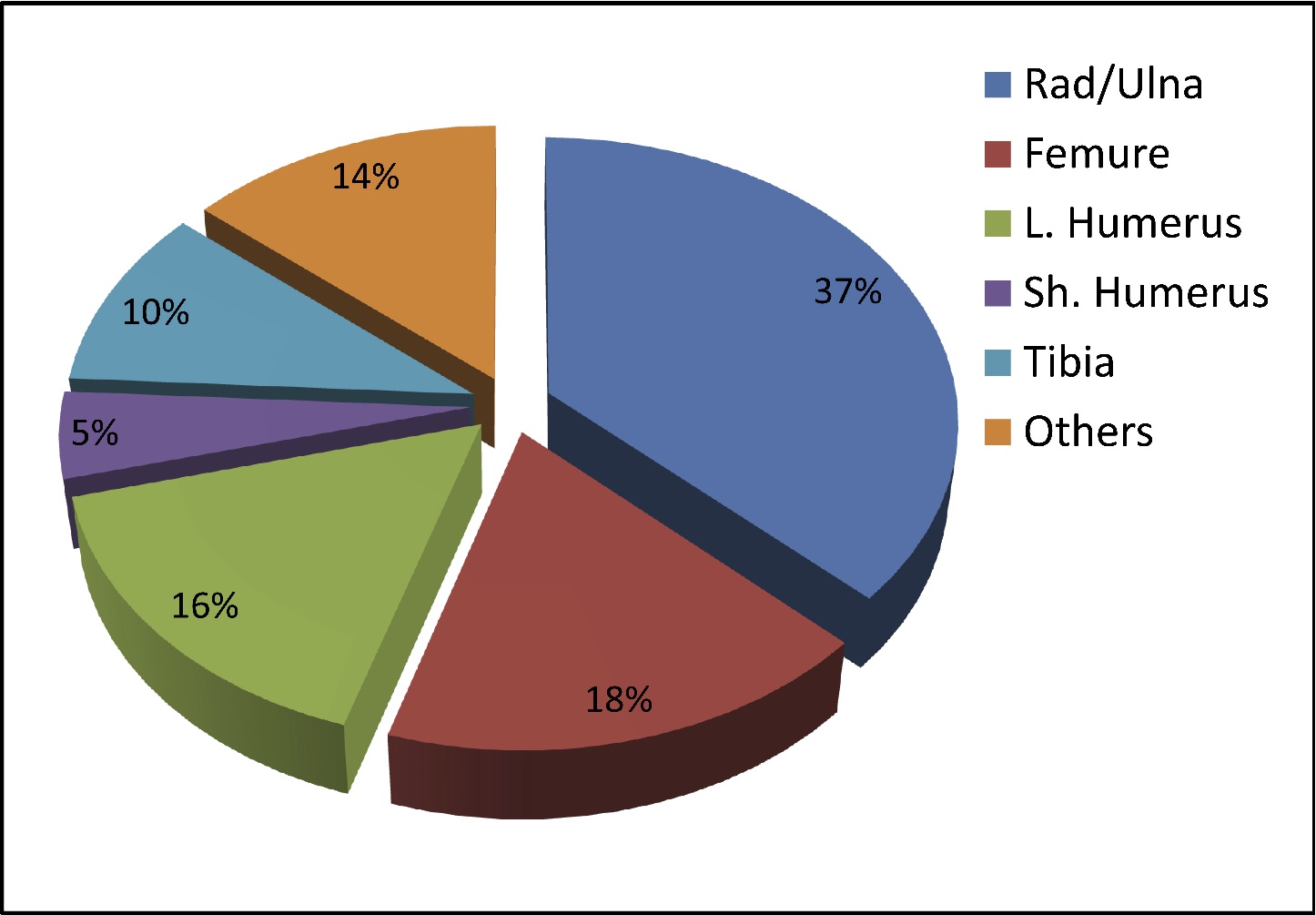
Figure 2: Distribution of Fractures
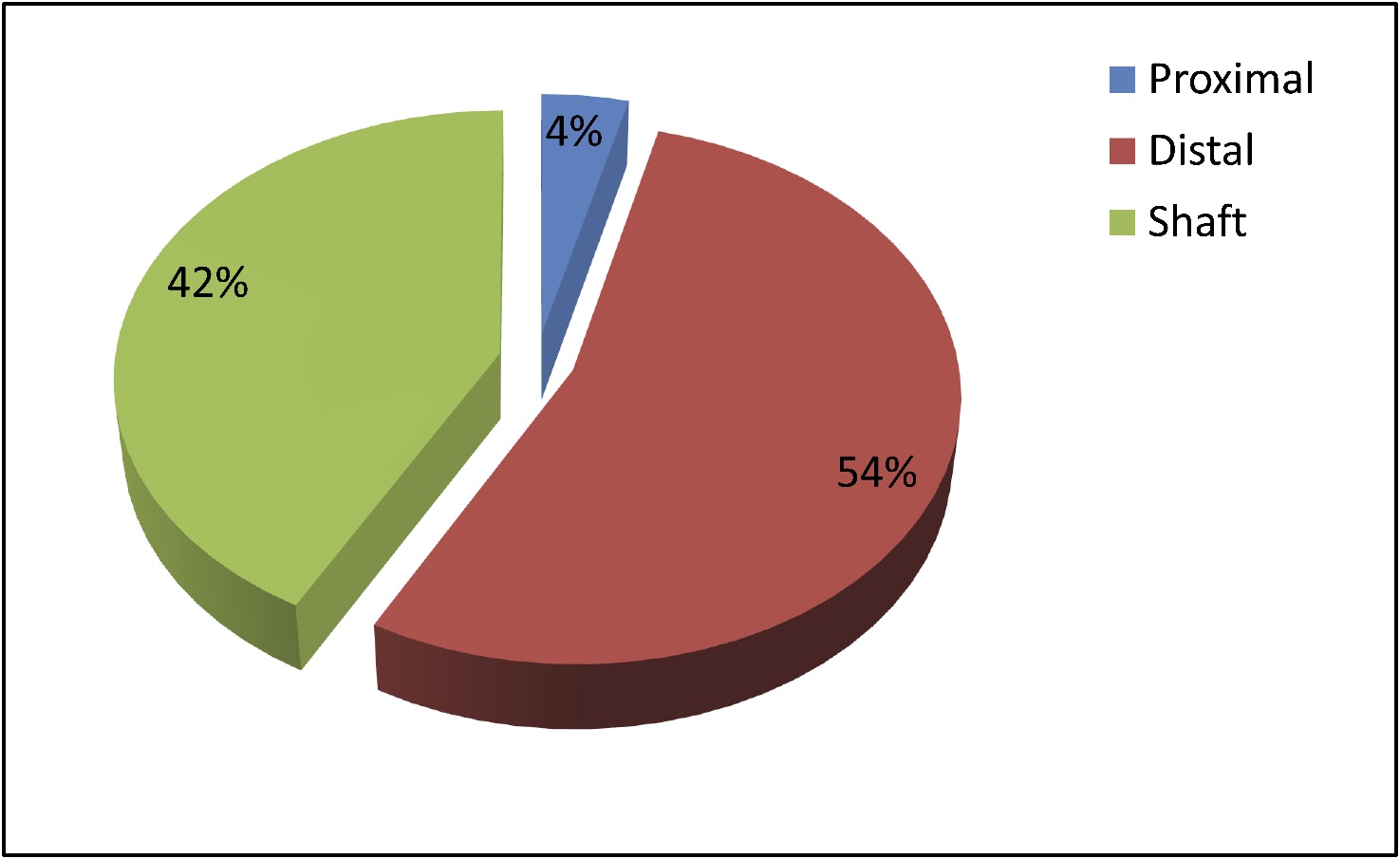
Figure 3: Site of fracture of radius
The distribution of radius fracture and the distribution of the hand and foot fractures are demonstrated in Figs. 3 and 4 respectively. The cause of fractures was diverse. In descending order, most of the fractures were sustained from falls 168 (62.3%), followed by road traffic accident 93 (34.4%), and sports related injuries 9 (3.3%). (Fig. 4)
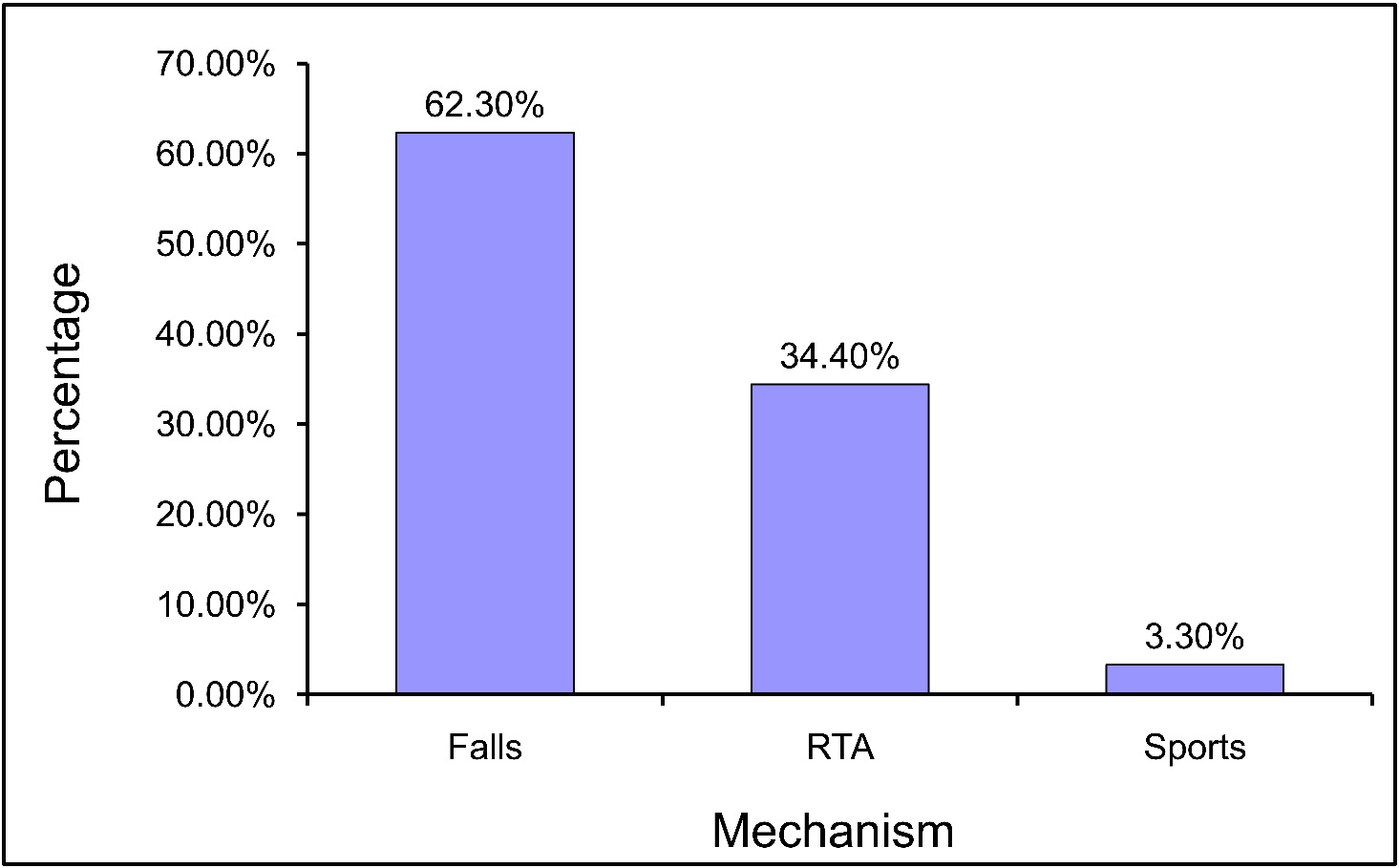
Figure 4: Mechanism of Injury
Fractures of the distal extremity were seen commonly as upper limb shaft fracture. Those resulting from high energy trauma were reported in the lower extremity and in older children. In all fractures, boys outnumbered girls, except in the age group of 1 year-olds where girls outnumbered boys. There were 11 infants (4 boys, 7 girls) with fractures of the shaft humerus, clavicle, femur and forearm bones treated conservatively. Seasonal variation in the admission rate was observed with a peak admission rate during the summer holiday between July and September, (Fig. 5). The seasonal variation in admission was statistically significant (p<0.001).
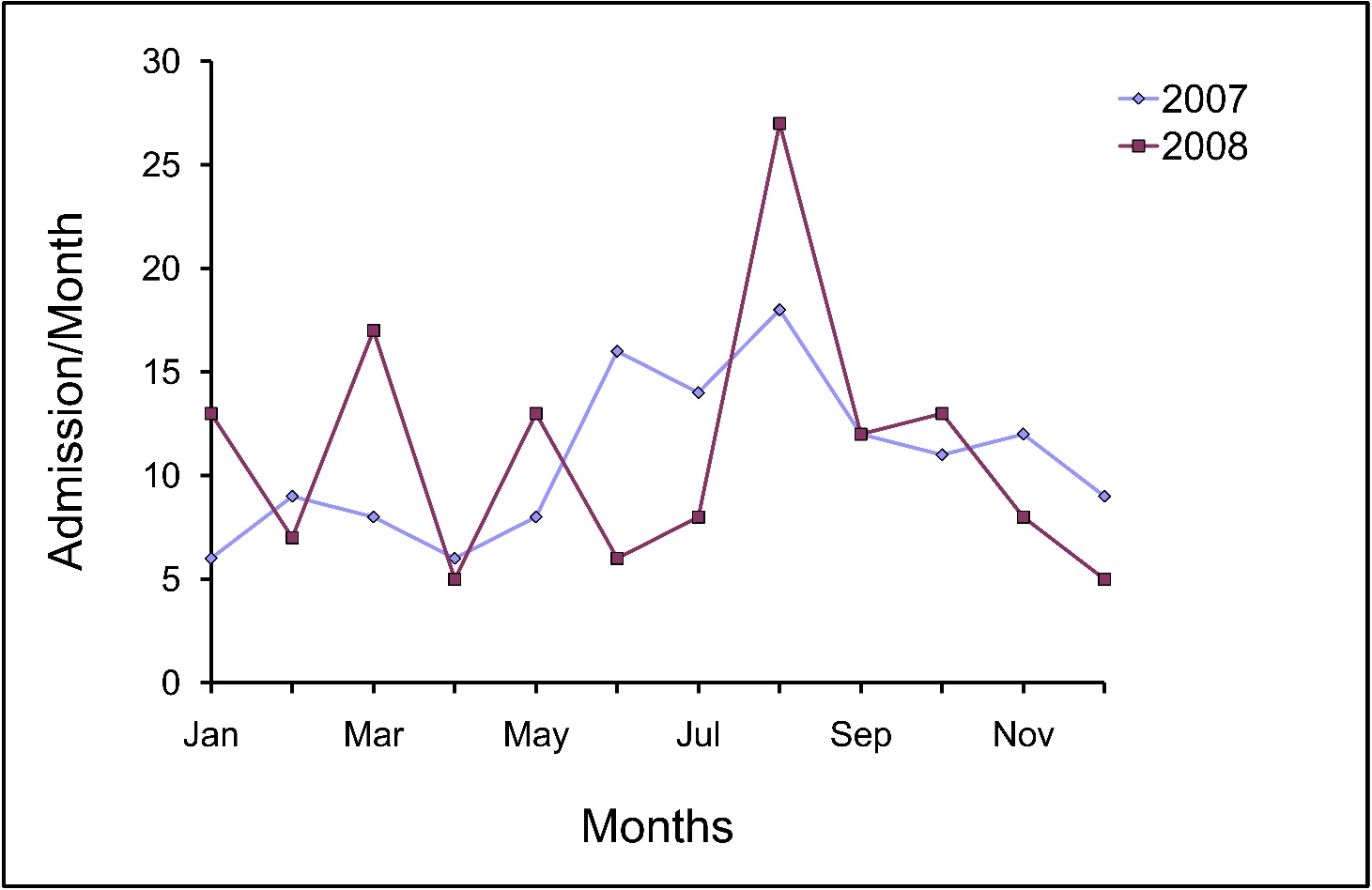
Figure 5: Seasonal Variation in Admission
The management of fracture is depicted in Table 1. In 188 children (69.6%), the treatment was in the form of operative intervention performed under general anaesthesia. Eighty-two children (30.3%) were managed conservatively with plaster slab/ cast, traction with hip spica. None of the patients required second operation during the initial admission. There was no reported mortality and all 270 children were discharged.
The femoral shaft fractures were managed in 30 cases by conservative management, skin traction followed by hip spica application and in 18 cases, operative intervention was done in the form of plating (11 cases), TIN (4 cases) and K-wire fixation (3 cases), (Table 2). All displaced forearm and distal radius fractures were managed by K-wire fixations.
Table 1: Primary Treatment of Fractures
| Primary Management |
No. of Children |
Percentage |
| Traction/POP |
52 |
19.2 |
| Traction/Hip spica |
30 |
11.1 |
| External/Internal Fixation |
188 |
69.6 |
Table 2: Management of femoral shaft fractures
| Primary Treatment |
No. of Patients |
Hospital stay (mean) |
Complication (shortening 2-3 cm) |
| Skin traction/Hip spica |
30 |
22.3 |
7 cases |
| ORIF with plating |
11 |
7.9 |
Nil |
| CRM with ESIN |
4 |
2.5 |
Nil |
| CRM with K-wire |
3 |
2.2 |
Nil |
In the current study, complications such as; neuropraxia of the median and ulnar nerve was observed in 5 (1.8%) patients with supracondylar fracture humerus, and in patients with stiff elbows and knees in 3 (1.1%) cases which on follow-up recovered in 4-6 weeks. Residual shortening of the femur about 2-3 cm without any functional disability was observed in 7 (23.3%) cases of fracture shaft femur treated conservatively. (Table 3)
Table 3: Complications recorded in our study group.
| Complications |
Total (%) |
| Failed conservative management |
7 (2.5%) |
| Neuropraxia upper limb |
5 (1.8%) |
| Stiff knee/elbow |
3 (1.1%) |
| Residual shortening in femur # |
7 (23.3%) |
In this study, 7 children (2.5%) were readmitted for a second time for secondary fracture stabilization after failure of conservative management. These patients had sustained fractures of forearm, distal radius, shaft humerus, and femur as there was loss of initial fracture position after closed manipulation and plaster immobilization. These patients required operative stabilization to achieve anatomical reduction and alignment. Readmissions accounted for further 20 bed occupancy days.
Salvage internal fixation in the form of K-wires or plating was employed after failure of conservatively treated fractures of distal radius (n=1), forearm fracture (n=3), humerus (n=2) and femur (n=1).With exception of patients with fracture of the shaft femur, most of the children were discharged within 72 hrs of admission. The median length of stay in hospital after fracture was 1.5 days (range 1- 25 days) and a total of 1730 beds were occupied over the period of 2007-2008. In 48 patients with fracture of the shaft femur (median stay of 19.2 days) occupied more beds (888) than 100 patients with radius and ulna fractures (median stay of 1.6 days) with bed occupancy of 194. (Table 4)
Table 4: Comparative cost from hospital stay for fracture femur and forearm fracture treatment
| Fracture |
Patients |
Mean stay (days) |
Cost @10 OMR/day |
| Femur |
48 |
19.2 |
9216 |
| Forearm |
100 |
1.6 |
1600 |
This variation was due to the majority of children with fractured femur being treated conservatively, in contrast to forearm fractures which were treated in nearly all patients at the outset by operative fracture stabilization accounting for short inpatient stay. (Table 3)
In terms of associated injuries, 43 (16%) patients with associated injuries of the head, chest, abdomen and face (Table 5) were admitted and managed by general surgeons. Fractures in these cases were managed under orthopedic care. While hand and foot injuries accounted for 37 (13.7%) cases. (Table 6)
Table 5: Pattern of associated injuries in our study
| Injuries |
Total (%) |
| Head injuries |
11 (4.07%) |
| Facial injuries |
4 (1.5%) |
| Cervical spine injuries |
2 (0.75%) |
| Chest injuries |
6 (2.2%) |
| Abdominal trauma |
5 (1.85%) |
| Pelvis fracture |
3 (1.1%) |
| Others |
10 (3.7%) |
| Dislocations |
2 (0.75%) |
| Total |
43 (16%) |
Table 6: Distribution of Hand and Foot injuries
| Distribution |
Percentage |
| Metacarpal fractures |
1% |
| Phalanx fractures |
1.8% |
| Epiphyseal injuries of phalanges |
3.5% |
| Ankle injuries |
5.5% |
| Metatarsal and phalanx injuries |
2.0% |
Discussion
Trauma is the commonest cause of morbidity and mortality in a population age less than 19 years.2 This audit is the first of its type in Oman, and there is no report of any such audit in the literature from any other Gulf countries. It is really difficult to assess the true incidence of limb fractures in children admitted for definitive management due to problems in data collection from hospital inpatient records, which varies widely in different countries. We were fortunate to have a computer based data bank, which tackled such problems of data discrepancies, however the incidence of human error cannot be ruled out. The reported admission rates are comparable to other reported series in literature.3-5
Variation if any could be due to local provisions of hospital service for fracture management, socioeconomic factors or health infrastructure, rather than true epidemiological differences in fracture incidence. The audit identified a marked seasonal variation in the admission rates which have important implications in staffing and bed availability. The audit further demonstrates an increase in admission during the summer with a trough in winter which is also reported in other studies, where a correlation between admission of children with fractures and sunshine hours has been documented.5-7
The mean age of the patients in our series was 7.2 years, which is similar to other studies.3,8 Comparative cost incurred in hospital stay was considerably more in patients with fracture of the shaft femur compared to patients with forearm fractures. Complications recorded were residual shortening of 2-3 cm in 7 (23.3%) patients with fracture shaft femur treated conservatively without functional disability, Neuropraxia in 5 (1.8%) cases. The fracture pattern shows the predominance of upper limb fractures (60.2%), of which 37% were forearm fractures followed by lower limb fractures accounting for (38.8%), then fractured femoral shaft (17.8%), followed by fractured tibia (10.3%). Similar fracture patterns have been reported in other studies.4-6
In the current study, it was apparent that falls accounted for a majority of fractures followed by road traffic accidents, which is in agreement with many studies.2,6,9 However, other studies have accounted road traffic accidents to be the major cause of pediatric fractures.4,8 Deakin et al. reported sports related injuries to be responsible for the majority of lower limbs fractures, while falls accounted for the majority of upper limb fractures.5 The differences in the etiology can be attributed to sociocultural differences in different countries, where the studies were conducted.
Male children accounted for the majority of patients in our series (3:1 ratio), which is similar to other studies, this could possibly be explained by the fact that male children are more active and adventurous.3-5,8 There were only 4 (1.5%) patients with open fractures (Gustillo types 1&2), which were managed by initial wound debridement and progressed to healing without any problem.
In our series, the most common site of fracture was observed in the forearm bones followed by the shaft femur, lower end humerus and the tibia respectively. This is consistent with most other studies in the literature, where distal radius fractures followed by elbow injuries being the common fractures to the tune of 35-60%.3,5,9-11 This is explained by the fact that children fall with outstretched arms. Femur fractures which account for more morbidity in children were recorded in 17.8% cases in this audit. There are few studies where femur fracture is the most common injury in the pediatric population.4,6,8 This can be explained by the fact that vehicular accidents was the common mode of injury in these studies, especially bumper impact which usually affect the lower limbs.
In the past, conservative management of pediatric fractures was predominant, but operative intervention in certain fracture is now the method of choice. However, treatment modalities may vary in different centres. Surgical intervention was performed in 70% of cases, mostly in fractures of the forearm, elbow, femur and ankle in the form of K-wire, TIN, and Plating. Our operative rates were higher compared to other studies.6,8
Displaced radial fractures from other studies have reported a 7-13% risk of re-displacement after initial conservative management, irrespective of quality of cast immobilization and surgeons’ experience.12,13 This problem of re-displacement and unplanned readmission were subsequently avoided in our cases, largely by adopting selective use of percutaneous K-wire stabilization of all displaced distal radius, and diaphyseal fractures.
Early operative intervention helped prevent unplanned readmissions, overloading of the ward and alleviating undesirable stress on both the family and the patient.
In the current study, it was observed through serial radiological analysis that accuracy of reduction and maintenance of rotational alignment is important for final anatomical outcome of any fracture and that treatment has to be tailored to individual fracture pattern, while keeping in mind the various sociocultural factors prevalent in the region. Parents in the gulf are keen on anatomical fracture reduction from the outset and are not willing to accept the concept of remodeling or conservative management.
The specific areas of concern which were identified during this audit and where management could be improved were mainly; 1) Prolonged inpatient stay for femoral shaft fractures, 2) Unplanned admissions and surgery, and 3) Cost impact of prolonged inpatient stay.
The prolonged inpatient stay and increase in bed days in this series was found in patients with femoral shaft fractures, which is supported by previous studies.5,14 Femoral shaft fractures has an incidence of 2% of all pediatric fractures, however, it puts a lot of strain on hospital resources than other fractures, and our hospital is no exception to this fact.14 At Nizwa hospital, we have rationalized and streamlined fracture management in children with a goal for early and safe hospital discharge by early intervention in the form of percutaneous external fixation, flexible nails, plating and early hip spica depending on the age of the child, type and location of the fracture. This has resulted in shorter hospital stays, which benefit all parties, namely; the patients, families and the hospital.
Although salvage internal fixation of pediatric fractures was not a problem in our cases, it is gaining importance and this is evident by the relatively high incidence in certain reported series.6,12-14 This is primarily due to uncertainty in primary management of particular fractures. This calls for definitive primary treatment protocols for different fractures.
Conclusion
The burden of fracture in children in Oman is frequently associated with morbidities. The injuries are preventable and pediatric trauma prevention strategies directed at parents and children with changes in lifestyle and by overcoming obstacles such as ignorance, illiteracy and inadequate resources are imperative. Public enlightenment, provision of pedestrian pathways, adequate and safe building constructions will help reduce the burden of such fractures in developing countries, where the burden of childhood disease obscures trauma care.
Acknowledgments
The authors reported no conflict of interest and no funding was received for this work.
|