
Figure 1: Radiograph of the chest at the time of admission.
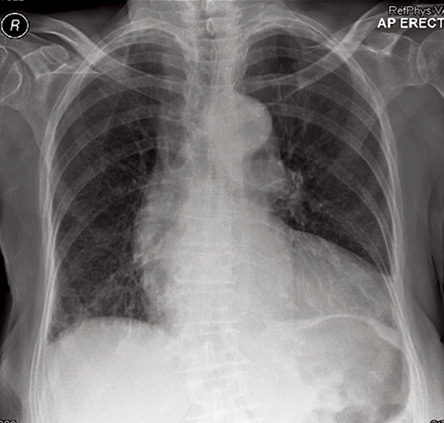
Figure 2: Radiograph of the chest after two days of inpatient treatment
Clinical examination revealed elevated jugular venous pressure, minimal pedal edema, a systolic cardiac murmur and bibasal lung crackles. An electrocardiograph demonstrated left bundle branch block and left axis deviation. A chest radiograph revealed the abnormality shown by the arrow in Figure 1 which disappeared after two days of in-hospital treatment [Figure 2].
Question
1.What is the clinical diagnosis?
Answer
1.Cardiac enlargement, pulmonary edema and presence of a tumor-like mass.
discussion
The chest radiograph showed cardiac enlargement, pulmonary edema (“bat wing” appearance in the lungs), and a tumor-like mass in the right mid-zone [Figure 1, arrows]. Echocardiography revealed moderate aortic regurgitation and a left ventricular ejection fraction of 35%. She was managed with oxygen, intravenous furosemide and oral ramipril leading to rapid improvement of symptoms. A chest radiograph two days later showed disappearance of the tumor and complete resolution of pulmonary edema [Figure 2].
Interlobar effusion in the horizontal lung fissure secondary to pulmonary edema rarely gives rise to a radiological pseudotumor appearance. Prompt resolution of the pseudotumor (also named a phantom tumor) with the improvement of cardiac failure is the hallmark of this condition.1,2
Pulmonary venous congestion, initially in the upper lung zones (referred to as upper lobe venous diversion) is the earliest manifestation of pulmonary edema. As the pulmonary venous pressure increases (usually >20mmHg), fluid accumulates in the horizontal fissure and Kerley B lines (thickened inter-lobular septa) develop near the costophrenic angles.3 Frank pulmonary edema with a “bats wing” appearance in the lungs, bilateral pleural effusions, and alveolar consolidations may occur in the advanced stages. Cardiac enlargement (cardiothoracic ratio >50%) may or may not be present depending on the duration and the severity of hemodynamic disturbance that caused the pulmonary edema.3
references
- Alderisio WG. Images in cardiovascular medicine. Vanishing tumor. Circulation 2007 Apr;115(13):e381-e382.
- Ardic I, Yarlioglues M, Celik A, Kaya MG. Vanishing or phantom tumor of the lung. Tex Heart Inst J 2010;37(6):730-731.
- Davies MK, Gibbs CR, Lip GY. ABC of heart failure. BMJ 2000 Jan;320(7230):297-300.